
The freezing of ovarian tissue, also known as **O**varian **T**issue **C**ryopreservation (OTC), is an experimental type of fertility preservation, used predominantly by female cancer patients who would otherwise likely become infertile following treatment. **How is OTC performed?** ------------------------- Part or all of the ovary is removed using [](https://nabtahealth.com/what-is-a-laparoscopy/)[laparoscopy](https://nabtahealth.com/glossary/laparoscopy/). If the entire ovary is removed it may be cryopreserved whole, otherwise it is cut into very thin slices, between 0.3 and 2mm, which are frozen and stored until required. The tissue is thawed and re-transplanted, either into the pelvic region (orthotopic) or elsewhere in the body (heterotopic). **Part vs whole ovary?** ------------------------ It is not always necessary to remove the whole ovary, although your doctor might choose to if they anticipate complete ovarian failure. Often only the outer layer will be taken, this is known as the ovarian cortex. There are a large number of immature eggs (oocytes) located in primordial follicles in this part of the ovary. This means that taking a small volume of tissue could potentially provide hundreds of oocytes for subsequent fertility treatment. The advantage of taking the whole ovary is that there is less chance of tissue ischemia (where the blood supply is decreased, resulting in reduced oxygen supply to the tissue), as blood flow can be maintained, or rapidly restored (revascularisation), using the vascular pedicle. Following re-transplantation, the vascular pedicle ensures adequate oxygenation of the transplanted tissue, reducing the likelihood of transplant failure. However, there can be challenges with cryopreserving it in its entirety and, if anything goes wrong, survival of the entire ovary could be compromised. **Slow freezing vs vitrification?** ----------------------------------- Work to establish the optimal method of freezing resected ovarian tissue is on-going. The most widely used method is the slow freezing of the tissue in a step-by-step process until it reaches -140°C, at which point it is stored in liquid nitrogen. Slow freezing reduces the formation of ice crystals, which can damage the ovarian cells. Vitrification is a newer technique that uses ultra-fast cooling with a higher concentration of cryoprotectant. It is quick and relatively easy to perform, with no requirement for expensive equipment. However, so far it is not widely used and there is limited data on its effectiveness. **Orthotopic vs heterotopic** ----------------------------- Determining the best transplant site for your cryopreserved ovarian tissue largely depends on your reason for undergoing OTC. If you hope to fall pregnant naturally, your only option is to undergo an orthotopic transplant. In this procedure the cryopreserved ovarian tissue is transplanted back into the pelvic region. Strips of tissue are transplanted either onto the surface of the remaining ovary, or into the pelvic peritoneum. The close proximity to the [fallopian tubes](https://nabtahealth.com/glossary/fallopian-tube/) means natural pregnancy is possible. However, the size of the transplant site restricts the number of fragments that can be transplanted. Menstrual cycles typically resume 4-9 months after OTC, which aligns closely with the time it takes for normal follicular growth and [oocyte](https://nabtahealth.com/glossary/oocyte/) maturity. This suggests that following OTC and re-transplantation the ovarian eggs start to develop normally. The lifespan of transplanted ovarian grafts is variable, the longest to date has been seven years. During a heterotopic transplant the ovarian tissue is re-transplanted elsewhere in the body. Frequently used sites are the forearm, abdomen wall and chest wall. Provided the transplant is successful, the transplanted ovarian tissue should start to produce hormones again, minimising any unwanted menopausal symptoms; however, pregnancy will only be possible using egg retrieval processes and artificial reproductive techniques/technologies (ARTs). The advantage to this type of transplant is that the graft can be placed in a location that allows for ease of access, so that maturing follicles can be monitored and retrieved if required for [IVF](https://nabtahealth.com/glossary/ivf/) and the transplanted tissue can be checked for signs of cancer recurrence. Aside from the fact that natural pregnancy is not possible following this type of transplant, the main disadvantage is that the transplanted tissue is less likely to survive due to difficulties reestablishing a blood supply. **Benefits to OTC** ------------------- For those women facing sudden, unexpected or premature ovarian failure, OTC provides an option for maintenance of fertility. Unlike embryo or egg freezing, where a complex harvesting process yields a “normal range” of 8-15 eggs per procedure; removing the ovarian cortex results in the harvesting of hundreds to thousands of immature oocytes. Furthermore, it is a simpler process, there is no need to wait for a particular time in the cycle and therefore, the procedure can be performed with minimal notice period. The additional benefit to this is that any cancer treatment is not delayed as a result. OTC is the only fertility preserving option for girls who have not yet gone through [](https://nabtahealth.com/what-is-puberty/)[puberty](https://nabtahealth.com/glossary/puberty/). This is because they do not yet have mature eggs to harvest directly. **Negatives to OTC** -------------------- Despite its potential, to date, OTC remains an experimental procedure. It is not yet endorsed by the American Society for Reproductive Medicine as a fertility preserving technique. There is hope that with more robust data, it will become more widely implemented in the clinical setting. There is a risk that re-transplanting grafted tissue will reintroduce unwanted malignancies. There is more chance of this with blood-borne cancers, such as the leukaemias. **Use of OTC for cancer patients** ---------------------------------- The nature of many types of cancer treatment means that they are toxic to [germ cells](https://nabtahealth.com/glossary/germ-cells/). Whilst chemoradiotherapy often does an excellent job of killing malignant cells, it can have a quite catastrophic effect on other cells of the body too. Learning that you have cancer and are likely to be rendered infertile by the treatment you receive is a huge psychological hurdle to overcome. In fact, the National Institute of Clinical Excellence (NICE) guidelines from the UK state that fertility preservation should be a part of the management of all cancer patients. OTC has the potential to be of significant benefit to those facing [cancer-induced](https://nabtahealth.com/causes-of-female-infertility-cancer/) [infertility](https://nabtahealth.com/glossary/infertility/). However, it might not just be a case of rectifying [infertility](https://nabtahealth.com/glossary/infertility/). Ovarian failure and a sudden drop in [oestrogen](https://nabtahealth.com/glossary/oestrogen/) and [progesterone](https://nabtahealth.com/glossary/progesterone/) production essentially places the body in a menopausal state. This triggers a range of symptoms that can be challenging to deal with both physically and emotionally, for example, [hot flushes](https://nabtahealth.com/glossary/hot-flushes/), difficulty sleeping, [vaginal dryness](https://nabtahealth.com/5-reasons-why-you-may-be-experiencing-vaginal-dryness/) and reduced libido. OTC following by orthotopic transplantation reestablishes normal ovarian activity in as many as 95% of cases. This has the potential to alleviate challenging menopausal symptoms, without the need to rely on hormone replacement therapy ([HRT](https://nabtahealth.com/glossary/hrt/)). **Alternative uses** -------------------- OTC is most strongly associated with the restoration of fertility in those who need to undergo life-saving, ovary-toxic cancer treatment. However, it has other potential uses for those with [benign](https://nabtahealth.com/glossary/benign/) disease, such as recurrent [](https://nabtahealth.com/can-endometriosis-make-it-harder-to-get-pregnant/)[endometriosis](https://nabtahealth.com/glossary/endometriosis/) and advanced [ovarian torsion](https://nabtahealth.com/what-is-ovarian-torsion/). It has the potential to be used prophylactically in those with a history of [primary ovarian insufficiency](https://nabtahealth.com/causes-of-female-infertility-failure-to-ovulate/) ([POI](https://nabtahealth.com/glossary/poi/)) or with [auto-immune diseases](https://nabtahealth.com/causes-of-female-infertility-autoimmune-and-immune-mediated-disorders/). There is also the option to use OTC as a means of postponing the [menopause](https://nabtahealth.com/glossary/menopause/). With life expectancy increasing, it is now estimated that a high number of women will spend a significant proportion of their life post-[menopause](https://nabtahealth.com/glossary/menopause/). There are certain risks associated with this from both a health and a quality of life perspective. Postmenopausal women are at greater risk of experiencing [](https://nabtahealth.com/osteoporosis-and-menopause/)[osteoporosis](https://nabtahealth.com/glossary/osteoporosis/), cardiovascular disease and depression; and [HRT](https://nabtahealth.com/glossary/hrt/) is not suitable for everyone. Securely cryopreserving a large population of ovarian follicles, which when grafted back into the human body would start producing the female sex hormones, is one way to delay the onset of [menopause](https://nabtahealth.com/glossary/menopause/). However, whilst the idea makes sense in theory, as an experimental procedure, OTC is not currently endorsed to be used in this way. **Current status** ------------------ As described above, OTC has a lot of potential. So far the technique has resulted in more than 130 live births. There are technical challenges still to overcome. The protocols for freezing the resected tissue need optimising because current methods result in a lot of empty follicles, possibly as a result of ice crystal formation. Improving the viability of the follicles would increase the lifespan of the grafted tissue. There also needs to be further consideration of who could benefit from the procedure. Going forward, is this a feasible way of postponing the onset of the [menopause](https://nabtahealth.com/glossary/menopause/) for completely healthy women? Or, is it something that should be kept and optimised for use as a fertility preservation technique for those facing imminent, premature [infertility](https://nabtahealth.com/glossary/infertility/)? It is best if you try [](https://nabtahealth.com/product/perimenopause-test/)[Perimenopause](https://nabtahealth.com/glossary/perimenopause/) test to understand more on your health. Nabta is reshaping women’s healthcare. We support women with their personal health journeys, from everyday wellbeing to the uniquely female experiences of fertility, pregnancy, and [menopause](https://nabtahealth.com/glossary/menopause/). Get in [touch](/cdn-cgi/l/email-protection#a0d9c1ccccc1e0cec1c2d4c1c8c5c1ccd4c88ec3cfcd) if you have any questions about this article or any aspect of women’s health. We’re here for you. **Sources:** * Broekmans, Frank J. “Individualization of [FSH](https://nabtahealth.com/glossary/fsh/) Doses in Assisted Reproduction: Facts and Fiction.” _Frontiers in Endocrinology_, vol. 10, 26 Apr. 2019, doi:10.3389/fendo.2019.00181. * Donnez, Jacques, and Marie-Madeleine Dolmans. “Fertility Preservation in Women.” _New England Journal of Medicine_, vol. 377, no. 17, 26 Oct. 2017, pp. 1657–1665., doi:10.1056/nejmra1614676. * “[Menopause](https://nabtahealth.com/glossary/menopause/): Symptoms.” _NHS Choices_, NHS, [www.nhs.uk/conditions/](http://www.nhs.uk/conditions/menopause/symptoms/)[menopause](https://nabtahealth.com/glossary/menopause/)/symptoms/. * “Ovarian Tissue Freezing.” _National Cancer Institute_, [www.cancer.gov/publications/dictionaries/cancer-terms/def/ovarian-tissue-freezing](http://www.cancer.gov/publications/dictionaries/cancer-terms/def/ovarian-tissue-freezing). * Rivas Leonel, Ellen Cristina, et al. “Cryopreservation of Human Ovarian Tissue: A Review.” _Transfusion Medicine and Hemotherapy_, vol. 46, no. 3, 9 Apr. 2019, pp. 173–181., doi:10.1159/000499054. * The Practice Committee of the American Society for Reproductive Medicine. “Ovarian Tissue Cryopreservation: a Committee Opinion.” _Fertility and Sterility_, vol. 101, no. 5, 31 Mar. 2014, pp. 1237–1243., doi:10.1016/j.fertnstert.2014.02.052.

* Charting your basal body temperature (BBT) is a way to understand where you are in your menstrual cycle, helping you to predict the exact point of [ovulation](https://nabtahealth.com/glossary/ovulation/). * Basal body temperature is your body temperature when it is at rest and it increases by around 0.3 – 0.6°C during [ovulation](https://nabtahealth.com/glossary/ovulation/). * Measuring basal body temperature can be done orally, vaginally or rectally and is best taken each morning, after sleep. * Vaginal monitoring is the most precise method with 99% accuracy and can be done using the [OvuSense vaginal thermometer](https://nabtahealth.com/product/cycle-monitoring-with-ovusense/) alongside the [Nabta app.](https://nabtahealth.com/our-platform/nabta-app) A woman’s menstrual cycle lasts from the first day of menstruation to the day before her next period starts. For women who have a very regular 28 day cycle, [ovulation](https://nabtahealth.com/glossary/ovulation/) will usually occur around day 15, which is approximately 2 weeks before the start of the next menstrual cycle. However, a ‘normal’ menstrual cycle can vary from 21 to 40 days, so determining the exact point at which [ovulation](https://nabtahealth.com/glossary/ovulation/) occurs is not that simple. It is, however, possible to use physiological cues (the way the body functions) to determine the likely start of [ovulation](https://nabtahealth.com/glossary/ovulation/); the body produces certain physical signs in response to fluctuating hormone levels and by accurately monitoring these, you may be able to deduce when you are most fertile. Approaches such as [observing cervical mucus](../cervical-discharge-through-the-menstrual-cycle) and measuring Basal Body Temperature (BBT) are types of fertility awareness-based methods that can be used for natural family planning. #### What is Basal Body Temperature? BBT is the temperature of the person at rest. During [ovulation](https://nabtahealth.com/glossary/ovulation/), the BBT usually rises by 0.3 – 0.6°C (0.5 – 1.0°F). By accurately recording the BBT every day, a woman may be able to determine if and when [ovulation](https://nabtahealth.com/glossary/ovulation/) occurred. Typical temperature fluctuations during a normal cycle: * The follicular phase of the cycle is the time before [ovulation](https://nabtahealth.com/glossary/ovulation/). BBT is influenced by [oestrogen](https://nabtahealth.com/glossary/oestrogen/) levels and [progesterone](https://nabtahealth.com/glossary/progesterone/) levels are low. Normal BBT range: 36.4 – 36.8°C (97 – 98°F). * One day before [ovulation](https://nabtahealth.com/glossary/ovulation/) there is a peak in luteinising hormone. BBT reaches its lowest point, known as the nadir. * After [ovulation](https://nabtahealth.com/glossary/ovulation/), [progesterone](https://nabtahealth.com/glossary/progesterone/) levels increase up to 10-fold.Temperature increases 0.3 – 0.6°C (0.5 – 1.0°F) and typically remains above 37°C for the next 10-14 days. This is known as the luteal phase of the cycle. * If fertilisation does not occur, [progesterone](https://nabtahealth.com/glossary/progesterone/) levels and BBT both reduce 1-2 days before menstruation starts. [](https://nabtahealth.com/wp-content/uploads/2019/09/Charting-Your-Basal-Body-Temperature-300x224-1.webp) It is important to always measure BBT in the same way, orally, vaginally, or rectally, using the same thermometer. Measuring under the armpit is not considered to be accurate enough. The best time to record BBT is first thing in the morning before undertaking any physical activity. Ideally, BBT measurements should be taken after at least 3-4 hours sleep. BBT can be affected by increased stress, illness, medication use, alcohol consumption and changes in time zone/circadian rhythm. It is not recommended to take measurements if you are using hormonal contraceptives, as the synthetic hormones will disrupt the normal ovulatory cycle. #### What can you use basal body temperature for? As a means of contraception, recording BBT is not without its drawbacks. At best it predicts peak fertility, with the rise in temperature indicating that [ovulation](https://nabtahealth.com/glossary/ovulation/) has occurred. To completely avoid pregnancy, a female would need to abstain from intercourse from the start of menstruation until 3-4 days after the rise in BBT. The most valuable use for BBT plotting is perhaps as a tool for determining the best time to have intercourse if trying to conceive. For those women who have regular periods, measuring BBT for 3-4 cycles can give a fairly accurate prediction of which days they are most fertile. Male [sperm](https://nabtahealth.com/glossary/sperm/) can survive for 5-7 days inside the female reproductive tract, but once [ovulation](https://nabtahealth.com/glossary/ovulation/) triggers the release of the female egg from the [ovaries](https://nabtahealth.com/glossary/ovaries/), the egg only has a 24 hour period of viability. This means that a female is fertile from 5 days before [ovulation](https://nabtahealth.com/glossary/ovulation/), to 2 days afterwards. Outside of this window, she cannot conceive. By the time the BBT spike is seen, the female is reaching the end of her fertile period for that month. #### Can measuring basal body temperature help fertility? The major benefits to using BBT to identify [ovulation](https://nabtahealth.com/glossary/ovulation/) are that it is low-cost, easily accessible (the only equipment you need are a thermometer and chart paper to plot your readings) and non-invasive. One means of improving the efficacy of BBT is to combine it with other fertility awareness-based methods, such as the cervical mucus method. This method is based on the theory that cervical secretions change throughout the menstrual cycle. Using these two approaches in combination is known as the symptothermal approach. BBT can also be tracked alongside using our [OvuSense device](https://nabtahealth.com/products/ovusense/), which is a realtime fertility monitor, aimed to predict [ovulation](https://nabtahealth.com/glossary/ovulation/) with 99% accuracy. The benefits of tracking your basal body temperature ---------------------------------------------------- Tracking your basal body temperature (BBT) is a simple and effective way to gain insights into your menstrual cycle and fertility. BBT is the lowest body temperature that you experience during a 24-hour period, and it can be measured using a basal body thermometer. By taking your temperature every morning at the same time and recording it, you can create a chart that shows any changes in your BBT throughout your menstrual cycle. **There are several benefits to tracking your BBT, including:** 1. Identifying [ovulation](https://nabtahealth.com/glossary/ovulation/): Your BBT typically rises slightly during [ovulation](https://nabtahealth.com/glossary/ovulation/), which is when an egg is released from the [ovaries](https://nabtahealth.com/glossary/ovaries/) and can be fertilized. By tracking your BBT, you can identify when you are most likely to be ovulating, which can help you plan or avoid pregnancy. 2. Monitoring your menstrual cycle: By charting your BBT over time, you can get a better understanding of your menstrual cycle and how it varies from month to month. This can be helpful for identifying any changes or irregularities in your cycle, which can be a sign of underlying health issues. 3. Assessing your fertility: Your BBT can provide valuable insights into your fertility, and tracking it over time can help you and your doctor assess your overall reproductive health. For example, if your BBT remains consistently high over several cycles, it could indicate that you are not ovulating, which can affect your ability to conceive. 4. Predicting [ovulation](https://nabtahealth.com/glossary/ovulation/): By tracking your BBT and identifying when it rises, you can predict when you are most likely to ovulate and plan accordingly. This can be helpful for those who are trying to conceive or avoid pregnancy. The [Nabta App](https://nabtahealth.com/our-platform/nabta-app/) can be used to record the Basal Body Temperature and store and plot the data. Nabta is reshaping women’s healthcare. We support women with their personal health journeys, from everyday wellbeing to the uniquely female experiences of fertility, pregnancy, and [menopause](https://nabtahealth.com/glossary/menopause/). Get in [touch](/cdn-cgi/l/email-protection#a1d8c0cdcdc0e1cfc0c3d5c0c9c4c0cdd5c98fc2cecc) if you have any questions about this article or any aspect of women’s health. We’re here for you. Don’t forget you can register [here](https://nabtahealth.com/my-account) to become a Nabta member free of charge. **Sources:** * NHS Choices, _NHS_, [https://www.nhs.uk/conditions/contraception/natural-family-planning/](https://www.nhs.uk/conditions/contraception/natural-family-planning/). * “Fertility Awareness-Based Methods of Family Planning.” ACOG, _Women’s Health Care Physicians_, [https://www.acog.org/Patients/FAQs/Fertility-Awareness-Based-Methods-of-Family-Planning](https://www.acog.org/Patients/FAQs/Fertility-Awareness-Based-Methods-of-Family-Planning). * Pallone, S. R., and G. R. Bergus. “Fertility Awareness-Based Methods: Another Option for Family Planning.” _The Journal of the American Board of Family Medicine_, vol. 22, no. 2, 2009, pp. 147–157., doi:10.3122/jabfm.2009.02.080038. * Su, Hsiu-Wei, et al. “Detection of [Ovulation](https://nabtahealth.com/glossary/ovulation/), a Review of Currently Available Methods.” _Bioengineering & Translational Medicine_, vol. 2, no. 3, 16 May 2017, pp. 238–246., doi:10.1002/btm2.10058.

A man will be diagnosed with a low [sperm](https://nabtahealth.com/glossary/sperm/) count if his semen sample contains fewer than 15 million [sperm](https://nabtahealth.com/glossary/sperm/) per milliliter. The medical term for this condition is oligozoospermia and it is one [reason for male](../causes-of-male-infertility) [infertility](https://nabtahealth.com/glossary/infertility/). Establishing the [prevalence of male](https://nabtahealth.com/articles/why-is-it-so-difficult-to-establish-the-prevalence-of-male-infertility/) [infertility](https://nabtahealth.com/glossary/infertility/) is challenging. However, abnormal [sperm](https://nabtahealth.com/glossary/sperm/) production, including low [sperm](https://nabtahealth.com/glossary/sperm/) counts, is considered to be one of the major contributing factors. Having a low [sperm](https://nabtahealth.com/glossary/sperm/) count does reduce the odds of a couple falling pregnant. However, it can still happen; after all, it only takes a single [sperm](https://nabtahealth.com/glossary/sperm/) to fertilise an egg. A female can only fall pregnant if she ovulates, which is the process by which an egg is released from the ovary. This happens about midway through her menstrual cycle; for a woman with a 28 day cycle, [ovulation](https://nabtahealth.com/glossary/ovulation/) will occur around day 15. This is when she is at her most fertile and conception is most likely to occur. However, [sperm](https://nabtahealth.com/glossary/sperm/) can survive for approximately five days inside the female body. For those who wish to maximise their chances of conceiving, it is worth having intercourse every day. That is, from at least four days prior to the expected date of [ovulation](https://nabtahealth.com/glossary/ovulation/). The released egg is only viable for fertilisation for 12-24 hours after [ovulation](https://nabtahealth.com/glossary/ovulation/). Intercourse after this time will not result in pregnancy. ##### Methods used; There are methods available to assist a female in determining if and when she has ovulated, including commercially available kits and the charting of [basal body temperature](https://nabtahealth.com/charting-your-basal-body-temperature-bbt/) (BBT). BBT will rise 0.5°C after [ovulation](https://nabtahealth.com/glossary/ovulation/). Knowing precisely when [ovulation](https://nabtahealth.com/glossary/ovulation/) is likely and timing intercourse accordingly, will further increase the chances of successful fertilisation. If a female’s cycles are irregular this may be more challenging. Often the cause of low [sperm](https://nabtahealth.com/glossary/sperm/) count in males is unknown, with hormones, medications, genetics and childhood conditions all thought to play a role. To further increase the likelihood of pregnancy without medical intervention, men may be encouraged to make certain [lifestyle changes](../environmental-factors-that-contribute-to-male-infertility). It is important to treat underlying medical conditions. Adopting a [better diet](../do-vitamins-and-other-nutritional-products-improve-sperm-count) and avoiding alcohol and smoking can help. Seeking help for the management of medical issues, such as [](../what-are-varicoceles)[varicoceles](https://nabtahealth.com/glossary/varicoceles/), genital infections and hormonal irregularities. Nabta is reshaping women’s healthcare. We support women with their personal health journeys, from everyday wellbeing to the uniquely female experiences of fertility, pregnancy, and [menopause](https://nabtahealth.com/glossary/menopause/). Get in [touch](/cdn-cgi/l/email-protection#463f272a2a270628272432272e23272a322e6825292b) if you have any questions about this article or any aspect of women’s health. We’re here for you. **Sources:** * “Low [Sperm](https://nabtahealth.com/glossary/sperm/) Count.” _Mayo Clinic_, 18 Sept. 2018, www.[mayoclinic](https://www.mayoclinic.org/).org/diseases-conditions/low-[sperm](https://nabtahealth.com/glossary/sperm/)\-count/diagnosis-treatment/drc-20374591. * Sengupta, P, et al. “The Disappearing Sperms: Analysis of Reports Published Between 1980 and 2015.” _American Journal of Men’s Health_, vol. 11, no. 4, July 2017, pp. 1279–1304., doi:10.1177/1557988316643383.

Diagnosed with Azoospermia will be made if no spermatozoa ([sperm](https://nabtahealth.com/glossary/sperm/) cells) are detected in two semen samples, taken 2-3 months apart. Azoospermia affects approximately 15% of infertile men and, if unexpected, can be quite an upsetting diagnosis to come to terms with. Fortunately, advances in modern medicine mean that a significant number of men who are in this position go on to successfully father children. Before determining which treatment will be most suitable, it is first important to establish whether it is a case of obstructive azoospermia (OA) or non-obstructive azoospermia (NOA). **Obstructive Azoospermia (OA)** -------------------------------- OA, affecting up to 40% of men with azoospermia, occurs when part of the reproductive tract is blocked. The testes are usually normal sized and hormone levels are in the normal range. The blockage can be acquired, for example by previous vasectomy or by surgery or trauma to that area of the body; or it can be congenital. The most well-known example of congenital [infertility](https://nabtahealth.com/glossary/infertility/) is due to [](../causes-of-male-infertility)[Cystic Fibrosis](https://nabtahealth.com/glossary/cystic-fibrosis/). Depending on the part of the reproductive tract affected, reconstructive surgery is an option. Blockages in the [epididymis](https://nabtahealth.com/glossary/epididymis/) or [vas deferens](https://nabtahealth.com/glossary/vas-deferens/) can be treated with vasoepididymostomy or vasovasostomy (also known as a reverse vasectomy). Obstruction of the ejaculatory duct can be treated with transurethral resection of the ducts, whereby a small incision is made in the ejaculatory duct, enabling [sperm](https://nabtahealth.com/glossary/sperm/) to reach the semen. In some cases, even if blockage removal appears to have been successful, additional techniques are implemented to aid fertilisation because the [sperm](https://nabtahealth.com/glossary/sperm/) is prone to poor [](../low-sperm-motility-asthenozoospermia)[motility](https://nabtahealth.com/glossary/motility/). If reconstructive techniques are not suitable or do not work, [sperm](https://nabtahealth.com/glossary/sperm/) retrieval techniques might be attempted. Examples include: – TESE: testicular [sperm](https://nabtahealth.com/glossary/sperm/) extraction – TFNA: testicular fine needle aspiration – PESA: percutaneous epididymal [sperm](https://nabtahealth.com/glossary/sperm/) aspiration – MESA: microsurgical epididymal [sperm](https://nabtahealth.com/glossary/sperm/) aspiration. The choice of technique largely depends on patient preference as well as local expertise. If initial attempts do not yield sufficient [sperm](https://nabtahealth.com/glossary/sperm/), the doctor can try to extract from an alternative location, often at the same time, meaning additional procedures are kept to a minimum. [Sperm](https://nabtahealth.com/glossary/sperm/) retrieval is successful in over 90% of OA cases. Once extracted the [sperm](https://nabtahealth.com/glossary/sperm/) can be used directly for intracytoplasmic [sperm](https://nabtahealth.com/glossary/sperm/) injection (ICSI) or cryopreserved for use at a later date. **Non-obstructive Azoospermia (NOA)** ------------------------------------- NOA usually occurs as a result of a testicular deficiency. The underlying pathologies are varied and include genetic and congenital abnormalities, [](../what-are-varicoceles)[varicoceles](https://nabtahealth.com/glossary/varicoceles/) (enlarged testicular veins), hormonal disorders, medications and toxin exposure. Often men with NOA will have abnormal testes and/or hormone levels. NOA is sometimes associated with specific microdeletions in the Y chromosome (AZFa and AZFb) that have a particularly poor prognosis in terms of [sperm](https://nabtahealth.com/glossary/sperm/) retrieval. Therefore, genetic testing for microdeletions in this region may be offered to these men to determine the likelihood of finding viable [sperm](https://nabtahealth.com/glossary/sperm/) prior to them undergoing any additional procedures. Men with NOA have fewer options available to them. Not all of the [sperm](https://nabtahealth.com/glossary/sperm/) retrieval techniques are suitable, but TESE can be used. If this is unsuccessful, microsurgical testicular [sperm](https://nabtahealth.com/glossary/sperm/) extraction (micro-TESE) can be attempted. This method requires a skilled practitioner and a general anaesthetic, but the advantages are that blood supply is preserved and the surgeon can deliberately identify and select larger [seminiferous tubules](https://nabtahealth.com/glossary/seminiferous-tubules/), i.e. those more likely to contain [sperm](https://nabtahealth.com/glossary/sperm/). [Sperm](https://nabtahealth.com/glossary/sperm/) is found in 40-50% of men with NOA, including men who are azoospermatic as a result of previous [chemotherapy](https://nabtahealth.com/glossary/chemotherapy/). Those men who have been diagnosed with concurrent [varicoceles](https://nabtahealth.com/glossary/varicoceles/) might want to consider undergoing a varicoceletomy, as this has been shown to improve ejaculate [sperm](https://nabtahealth.com/glossary/sperm/) levels in 20-55% of men with NOA. Ideally, [sperm](https://nabtahealth.com/glossary/sperm/) that is extracted from a man with NOA should be used fresh, as freeze-thawing compromises its stability and viability. When compared to OA [sperm](https://nabtahealth.com/glossary/sperm/), NOA [sperm](https://nabtahealth.com/glossary/sperm/) is more susceptible to DNA damage. Men who do have a genetic condition need to consider carefully the chances of passing it on to their offspring if they do undergo additional fertility treatment using their own [sperm](https://nabtahealth.com/glossary/sperm/). **Assisted Reproductive Techniques (ARTs)** ------------------------------------------- Once [sperm](https://nabtahealth.com/glossary/sperm/) is extracted the next step is to attempt to fertilise the female’s egg. The most well-known [ART](https://nabtahealth.com/glossary/art/) is in vitro fertilisation ([IVF](https://nabtahealth.com/glossary/ivf/)). During [IVF](https://nabtahealth.com/glossary/ivf/) the female’s eggs are extracted and mixed with her partner’s [sperm](https://nabtahealth.com/glossary/sperm/) in a petri dish. Once fertilised the eggs are placed back into the female’s [uterus](https://nabtahealth.com/glossary/uterus/). ICSI is a variant of [IVF](https://nabtahealth.com/glossary/ivf/) that involves injecting a single [sperm](https://nabtahealth.com/glossary/sperm/) into an egg. This is ideal in cases where only small quantities of usable [sperm](https://nabtahealth.com/glossary/sperm/) could be harvested using the techniques described above. ICSI fertilisation rates are 45-75% for OA and 20-65% for NOA. Live birth rates following successful ICSI fertilisation are 18-55% for OA and 8-35% for NOA. Whilst these figures may still seem low it is worth considering that advances in reproductive medicine are progressing rapidly and, prior to the development of microsurgical techniques and ICSI, men with NOA would have had no chance of fathering their own children, having to rely instead on donor insemination. Whilst azoospermia can seem like a fairly intimidating diagnosis, it is important to remember that lack of [sperm](https://nabtahealth.com/glossary/sperm/) does not equal complete sterility. Many men still produce [sperm](https://nabtahealth.com/glossary/sperm/) and the techniques for harvesting it are becoming more refined and as a result more effective. Regardless, both OA and NOA may benefit from surgical procedures to correct the problem. If surgery is successful, there is a good chance that fertilisation will be able to occur through normal intercourse, avoiding the need for stressful, costly [ART](https://nabtahealth.com/glossary/art/). It is important to consider that [ART](https://nabtahealth.com/glossary/art/) can be very stressful for the female as she undergoes artificial hormonal induction to retrieve eggs. All options should be discussed with a doctor, prior to making a decision. Nabta is reshaping women’s healthcare. We support women with their personal health journeys, from everyday wellbeing to the uniquely female experiences of fertility, pregnancy, and [menopause](https://nabtahealth.com/glossary/menopause/). Get in [touch](/cdn-cgi/l/email-protection#b3cad2dfdfd2f3ddd2d1c7d2dbd6d2dfc7db9dd0dcde) if you have any questions about this article or any aspect of women’s health. We’re here for you. **Sources:** * Esteves, S C, et al. “[Sperm](https://nabtahealth.com/glossary/sperm/) Retrieval Techniques for Assisted Reproduction.” _International Braz J Urol_, vol. 37, no. 5, 2011, pp. 570–583. * Katz, D J, et al. “Male [Infertility](https://nabtahealth.com/glossary/infertility/) – The Other Side of the Equation.” _Australian Family Physician_, vol. 46, no. 9, Sept. 2017, pp. 641–646. * Jungwirth A, et al. _European Association of Urology (EAU)_ guidelines on male [infertility](https://nabtahealth.com/glossary/infertility/). Arnhem, The Netherlands: European Association of Urology, 2015. Available at [https://uroweb.org/wp-content/uploads/17-Male-](https://uroweb.org/wp-content/uploads/17-Male-Infertility_LR1.pdf)[Infertility](https://nabtahealth.com/glossary/infertility/)\_LR1.pdf \[Accessed 31 March 2019\]. * “What Is Male [Infertility](https://nabtahealth.com/glossary/infertility/)?” _Urology Care Foundation_, [www.urologyhealth.org/urologic-conditions/male-](http://www.urologyhealth.org/urologic-conditions/male-infertility)[infertility](https://nabtahealth.com/glossary/infertility/). * Wosnitzer, M, et al. “Review of Azoospermia.” _[Spermatogenesis](https://nabtahealth.com/glossary/spermatogenesis/)_, vol. 4, no. e28218, 31 Mar. 2014, doi:10.4161/spmg.28218.

\***_According to Patient Feedback_** “Who are the best gynaecologists in Dubai? Can anyone recommend an OBGYN?” You asked us and we turned the question back to you. We have compiled the top 10 gynaecologists in Dubai, based only on real patient recommendations, experience and feedback. No healthcare professionals were questioned. Gathered from exemplary recommendations across Dubai social media forums, these top 10 gynaecologists in Dubai not only have a wealth of clinical expertise in their field, they also stand out for the overwhelmingly positive comments from their patients. #### **Dr Salma Ballal, Consultant Obstetrics and Gynaecology, [Genesis Healthcare Center](https://www.genesis-dubai.com/our_doctors/dr-salma-ballal/)** Having delivered well over 1000 babies, Dr Salma Ballal has extensive experience in managing normal and complex pregnancies and deliveries. Dr Salma trained in obstetrics and gynaecology with the UK’s NHS where she developed a strong interest in maternal medicine, high-risk pregnancies, and labour care. She completed advanced maternal medicine and labour ward practice training with the Royal College of Obstetrics and Gynaecology (RCOG) before moving to Dubai in 2014. Dr Salma was most recently at Mediclinic Parkview hospital before joining the Genesis Healthcare Center team. Dr Salma believes in open communication with her patients and that “women should be kept informed through every step of what is the most amazing experience in any woman’s life.” She also offers pre-pregnancy counselling to patients with complicated or traumatic pregnancy history. Patients describe Dr Salma as “refreshingly honest”, and “very safe hands”, saying she “totally respected my wishes”. #### **Dr Esra Majid, Consultant [Obstetrician](https://nabtahealth.com/glossary/obstetrician/) and [Gynaecologist](https://nabtahealth.com/glossary/gynaecologist/),** [**Kings’ College Hospital Dubai**](https://kingscollegehospitaldubai.com/dr/esra-mejid/) Based in Dubai since 2016, Dr Esra has built a reputation for her management of high-risk pregnancies and gynaecological conditions. She worked at Al Zahra Hospital Dubai, where she regularly received excellent feedback from her patients, before moving to King’s College Hospital Dubai. At Kings’ College Hospital Dubai Dr Esra “performs major surgical procedures, follow up of high-risk pregnancies and deliveries, along with natural and water births.” Dr Esra qualified in Baghdad and went on to complete her Board Certificate in Obstetrics and Gynaecology in Sweden. She worked at the teaching hospital Sundsvall County Hospital and as a specialist at Sodra Alv Bord Hospital in Gothenburg before moving to Dubai. Patients have praised Dr Esra for her expertise and skill, describing her as “straight to the point, warm and approachable.” #### **Dr Vibha Sharma, Specialist [Gynaecologist](https://nabtahealth.com/glossary/gynaecologist/),** [**Prime Medical Center**](https://www.primehealth.ae/prime-medical-centers/medical-centers/prime-medical-center-sheikh-zayed-road/dr-vibha-sharma) Working in Dubai since 2004, Dr Vibha is known for her commitment to supporting women with a range of gynaecological and women’s health problems. In the UAE she worked at Ministry of Health and Tertiary Care hospitals prior to joining Prime Medical Center. Dr Vibha specialises in areas of women’s health requiring specialist gynaecological expertise. Qualified in India at Jammu Medical College, Dr Vibha went on to do her post-graduate at King George’s Medical College in Lucknow. She worked at Queen Mary’s Hospital Lucknow and Willingdon and Batra Hospitals and Research Centre in New Delhi before moving to the Middle East. Patients have described Dr Vibha as “consistent”, “approachable”, and “professional”. **Dr Aisha Alzouebi, Consultant [Obstetrician](https://nabtahealth.com/glossary/obstetrician/) and [Gynaecologist](https://nabtahealth.com/glossary/gynaecologist/),** [**Mediclinic Parkview Hospital**](https://www.mediclinic.ae/en/corporate/doctors/1/aisha-alzouebi-dr.html) Dr Aisha Alzouebi has more than 15 years of experience in obstetrics and gynaecology in the UK and the UAE, with specialist expertise in “early pregnancy, management of complications in early pregnancy, family planning and sexual health, [benign](https://nabtahealth.com/glossary/benign/) open and laparoscopic surgery and hysteroscopy.” A member of the UK’s Royal College of Obstetricians and Gynaecologists (RCOG), Dr Aisha attended medical school at Sheffield University and completed her Masters in Surgical Education at Imperial College London. Patient social media feedback on Dr Aisha said, “she was brilliant”, “I would highly recommend her”, “Dr Aisha is great”. #### **Dr Reeja Mary Abraham, Specialist in Obstetrics and Gynaecology,** [**Medcare Women and Children Hospital**](https://www.medcare.ae/en/physician/view/reeja-mary-abraham.html) A specialist in high-risk pregnancies, Dr Reeja takes an “evidence-based” approach to complex and low risk gynaecological issues. Dr Reeja is based at Medcare Women and Children Hospital, where she also “performs and assists in major and minor gynaecological procedures”. A member of the Indian Medical Association (IMA) and the Kerala Federation of Obstetricians and Gynaecologists (KFOG), Dr Reeja began her medical career at Christian Fellowship Hospital in Oddanchatram, Tamil Nadu and worked in hospitals in Kerala and Tamil Nadu before moving to Dubai to work at Medcare Women and Children Hospital. Patients recommending Dr Reeja describe her as “kind and attentive”, “highly professional”, and “detail-oriented”. #### **Dr Nashwa Abulhassan, Head of Obstetrics and Gynaecology, Dr** [**Sulaiman Al Habib Hospital Healthcare City**](https://www.hmguae.com/doctor/dr-nashwa-abul-hassan/) Dr Nashwa is a specialist in normal and complex pregnancies and deliveries, as well as “acute gynaecology and early pregnancy complications management” based at Dr Sulaiman Al Habib Hospital Healthcare City. A member of the Royal College of Obstetricians and Gynaecologists (RCOG) and an accredited member of the British society of colposcopists and cervical pathologists, Dr Nashwa has more than 15 years of experience in the UK and the UAE. Dr Nashwa has been featured in the UAE media discussing pregnancy complications and was most recently in [Gulf News](https://gulfnews.com/uae/health/step-by-step-guide-to-dealing-with-covid-19-during-pregnancy-1.80112211), offering advice for pregnant women who have tested positive for Covid-19. Dr Nashwa’s patients describe her as “kind and caring”. #### **Dr Samina Dornan, Consultant [Obstetrician](https://nabtahealth.com/glossary/obstetrician/) and [Gynaecologist](https://nabtahealth.com/glossary/gynaecologist/) and sub specialist in Maternal Fetal Medicine, [Al Zahra Hospital](https://azhd.ae/doctors/dr-samina-dornan/#:~:text=Consultant%20Maternal%20and%20Fetal%20Medicine,London%20to%20come%20to%20Dubai.)** An established international voice on maternal and fetal health issues, Dr Samina Dornan has extensive experience in fetal medicine. At Al Zahra Hospital she works as a consultant [obstetrician](https://nabtahealth.com/glossary/obstetrician/) and gynecologist with a sub-specialty in Maternal Fetal Medicine. Dr Samina qualified at Queen’s University Belfast. She received a fellowship from the Royal College of Obstetricians and Gynaecologists (RCOG) in 2017 and is the “first female Maternal Fetal Medicine sub-specialist \[at RCOG\]” to work with patients in Dubai. Frequently quoted in the media, Dr Samina is “extensively published in complex twin pregnancies”. Patient feedback on Dr Samina is overwhelmingly positive, describing her as “wonderful”, “absolutely fantastic”, “caring” and “amazing”. #### **Dr Sarah Francis, Consultant Obstetrics and Gynaecology,** [**American Hospital Dubai and American Hospital Al Khawaneej Clinic**](https://www.ahdubai.com/doctors-profile/sarah-francis) With clinical expertise in general and [benign](https://nabtahealth.com/glossary/benign/) gynaecology, adolescent gynaecological issues, polycystic ovarian syndrome ([PCOS](https://nabtahealth.com/glossary/pcos/)), and low and high-risk pregnancies, Dr Sarah supports patients at American Hospital Dubai and American Hospital Al Khawaneej Clinic. A member of the Royal College of Obstetricians and Gynaecologists (RCOG), Dr Sarah qualified in Sierra Leone and practised in NHS hospitals and trusts across the UK before moving to the UAE. She worked with patients at Drs Nicholas and Asp clinics before joining the team at American Hospital. Patients say that Dr Sarah is “wonderful” and “exceptionally supportive”. #### **Dr Dragana Pavlovic-Acimovic, Specialist Obstetrics and Gynaecology,** [**Mediclinic Meadows**](https://www.mediclinic.ae/en/corporate/doctors/8/dragana-pavlovic-acimovic.html) Dr Dragana has “a special interest in obstetrics” and consults on “adolescent gynaecology, [menopause](https://nabtahealth.com/glossary/menopause/), family planning” and various gynaecological conditions. Dr Dragana qualified in Serbia and started her career at University Hospital Narodni Front in Belgrade, “the largest specialised obstetrics and gynaecology centre in South-East Europe”. She moved to Dubai in 2015 and worked at Drs Nicholas and Asp before joining Mediclinic. Patients’ experience with Dr Dragana is “great”. #### **Dr Alessandra Pipan, Consultant [Obstetrician](https://nabtahealth.com/glossary/obstetrician/) and [Gynaecologist](https://nabtahealth.com/glossary/gynaecologist/),** [**Mediclinic City Hospital**](https://www.mediclinic.ae/en/corporate/doctors/1/alessandra-pipan.html) With more than 30 years’ experience in gynaecology and obstetrics Dr Alessandra treats a range of gynaecological conditions, is a specialist in [infertility](https://nabtahealth.com/glossary/infertility/) and oncology, and works with high-risk pregnancies at Mediclinic City Hospital. A member of the Royal College of Obstetrics and Gynaecology (RCOG), the European Society of Reproduction and Embryology, and the European Society of Gynaecological Endoscopy, Dr Alessandra qualified at Cattolica University of Rome, Italy and has developed extensive sector experience in positions across the Italian and UAE healthcare institutions. Patients of Dr Alessandra have described her as “great” and “amazing”. \_\_\_ Nabta is reshaping women’s healthcare. We support women with their personal health journeys, from everyday wellbeing to the uniquely female experiences of fertility, pregnancy, and [](https://nabtahealth.com/glossary)[menopause](https://nabtahealth.com/glossary/menopause/). You can track your menstrual cycle and get [personalised support by using the Nabta app.](https://nabtahealth.com/our-platform/nabta-app/) Get in [touch](/cdn-cgi/l/email-protection#fc859d90909dbc929d9e889d94999d908894d29f9391) if you have any questions about this article or any aspect of women’s health. We’re here for you.

* Uterine [polyps](https://nabtahealth.com/glossary/polyps/) can arise in the neck of the [uterus](https://nabtahealth.com/glossary/uterus/), the [cervix](https://nabtahealth.com/glossary/cervix/) (cervical [polyps](https://nabtahealth.com/glossary/polyps/)) or the lining of the uterine cavity (endometrial [polyps](https://nabtahealth.com/glossary/polyps/)). * Relatively common, [polyps](https://nabtahealth.com/glossary/polyps/) are usually [benign](https://nabtahealth.com/glossary/benign/), often [asymptomatic](https://nabtahealth.com/glossary/asymptomatic/) and don’t need to be removed. * Two key symptoms of [polyps](https://nabtahealth.com/glossary/polyps/) are unusual bleeding (irregular periods, heavy periods, bleeding between periods) and [](https://nabtahealth.com/what-is-infertility/)[infertility](https://nabtahealth.com/glossary/infertility/). * Older women are more likely to develop [polyps](https://nabtahealth.com/glossary/polyps/). #### **What are [polyps](https://nabtahealth.com/glossary/polyps/)?** [Polyps](https://nabtahealth.com/glossary/polyps/) are the most frequently observed structural abnormality of the female reproductive tract, affecting up to 10% of the female population. They can range in size from a few millimeters to filling the entire uterine cavity, and will either lie flat against the lining of the [uterus](https://nabtahealth.com/glossary/uterus/) (sessile [polyps](https://nabtahealth.com/glossary/polyps/)), or project from the endometrium via a stalk (pedunculated [polyps](https://nabtahealth.com/glossary/polyps/)). The growth rate of [polyps](https://nabtahealth.com/glossary/polyps/) can also be highly variable; some will grow steadily over time, others will actually regress. [Polyps](https://nabtahealth.com/glossary/polyps/) are usually diagnosed using [transvaginal ultrasound](https://nabtahealth.com/glossary/transvaginal-ultrasound/) or [hysteroscopy](../what-is-a-hysteroscopy), with the latter technique considered to be the more accurate. An endometrial [biopsy](https://nabtahealth.com/glossary/biopsy/) will usually be performed to assess whether the [polyps](https://nabtahealth.com/glossary/polyps/) are [benign](https://nabtahealth.com/glossary/benign/). With few clinical symptoms, [polyps](https://nabtahealth.com/glossary/polyps/) are often only uncovered following investigative procedures for unexplained [infertility](https://nabtahealth.com/glossary/infertility/). In fact, the two main symptoms of [polyps](https://nabtahealth.com/glossary/polyps/) are: * [Abnormal uterine bleeding](../what-is-abnormal-uterine-bleeding) (irregular periods, heavy periods, spotting between periods) * [Infertility](https://nabtahealth.com/glossary/infertility/). [Polyps](https://nabtahealth.com/glossary/polyps/) have been implicated in up to 50% of cases of abnormal bleeding and [35% of](https://nabtahealth.com/causes-of-female-infertility-an-overview/) [infertility](https://nabtahealth.com/glossary/infertility/) cases. Premenopausal women are less likely to experience abnormal bleeding that is related to [polyps](https://nabtahealth.com/glossary/polyps/) than older women. #### **Risk factors and Causes of Uterine [Polyps](https://nabtahealth.com/glossary/polyps/)** It is not always known what causes [polyps](https://nabtahealth.com/glossary/polyps/) to develop. * **Age** is a major factor and [polyps](https://nabtahealth.com/glossary/polyps/) are rarely found in women below 30. Recent work suggests that [polyps](https://nabtahealth.com/glossary/polyps/) might exist in a latent state in younger women, with those that do form being more prone to regression as the cells of the endometrium undergo continual cycling. * **Medication**. Whilst the exact mechanisms that [lead](https://nabtahealth.com/glossary/lead/) to the formation of uterine [polyps](https://nabtahealth.com/glossary/polyps/) is unclear, there is a strong association between their development and [oestrogen](https://nabtahealth.com/glossary/oestrogen/). Women who are prescribed Tamoxifen or Hormone Replacement Therapy ([HRT](https://nabtahealth.com/glossary/hrt/)) are at increased risk of polyp formation. Tamoxifen is a partial [oestrogen](https://nabtahealth.com/glossary/oestrogen/) agonist used in the treatment of breast cancer. The incidence of endometrial [polyps](https://nabtahealth.com/glossary/polyps/) in women who have been prescribed tamoxifen is thought to be between 5 and 35%. [HRT](https://nabtahealth.com/glossary/hrt/) is frequently prescribed for menopausal women to alleviate some of the most uncomfortable symptoms. The oestrogenic effects exerted by tamoxifen on the [uterus](https://nabtahealth.com/glossary/uterus/), and the continuous, unopposed stimulation of the endometrium that occurs with [HRT](https://nabtahealth.com/glossary/hrt/), can both give rise to [oestrogen](https://nabtahealth.com/glossary/oestrogen/)\-dependent [polyps](https://nabtahealth.com/glossary/polyps/). Upon removal, these [polyps](https://nabtahealth.com/glossary/polyps/) have been found to contain increased numbers of [oestrogen](https://nabtahealth.com/glossary/oestrogen/) receptors. * **Obesity** is an additional risk factor for polyp development because adipose tissue contains high levels of an [enzyme](https://nabtahealth.com/glossary/enzyme/) called aromatase, which converts circulating [androgens](https://nabtahealth.com/glossary/androgen/) into oestrogens. * **Genetics**. Not all [polyps](https://nabtahealth.com/glossary/polyps/) are hormonally-driven. Apoptosis, or the process of controlled cell death, has been proposed as one of the regulatory mechanisms responsible for ensuring the endometrium is shed with each menstrual cycle. There is evidence that apoptotic activity is reduced in polyp tissue, which could explain why these growths are not shed with the rest of the endometrial lining during menstruation. Furthermore, chromosomal abnormalities and differing genetic activity have been found in some women with [polyps](https://nabtahealth.com/glossary/polyps/); particularly affected are those genes that regulate cell growth. Further work on the involvement of genes in polyp formation is required, to discern whether there is a familial, heritable component to the condition. * **[Inflammation](https://nabtahealth.com/glossary/inflammation/)** has also been proposed as a potential risk factor, with the suggestion that [polyps](https://nabtahealth.com/glossary/polyps/) occur as a result of localised tissue [inflammation](https://nabtahealth.com/glossary/inflammation/). #### **Polyp Removal** The [gold](https://nabtahealth.com/glossary/gold/) standard treatment approach for those [polyps](https://nabtahealth.com/glossary/polyps/) that are causing physical discomfort or contributing to difficulties in conceiving is for patients to undergo a hysteroscopic polypectomy. This is a relatively simple technique that involves removal of the polyp tissue. Cervical [polyps](https://nabtahealth.com/glossary/polyps/) can often be removed using forceps; larger endometrial [polyps](https://nabtahealth.com/glossary/polyps/) may require cauterisation. Once removed, the recurrence rate is relatively low and complications are rare. [](../what-is-a-dilation-and-curettage-and-why-is-it-done)[Dilation](https://nabtahealth.com/glossary/dilation/) and curettage (D&C) is an alternative technique sometimes used for the treatment of uterine pathologies. It is not the preferred approach for [polyps](https://nabtahealth.com/glossary/polyps/) removal due to the high possibility of missing [polyps](https://nabtahealth.com/glossary/polyps/) during the procedure. Women with [polyps](https://nabtahealth.com/glossary/polyps/) that are <10 mm in size are more likely to see natural regression over time and those who are [asymptomatic](https://nabtahealth.com/glossary/asymptomatic/) may prefer to avoid surgical management altogether. However, in approximately 1% of cases, [polyps](https://nabtahealth.com/glossary/polyps/) can become cancerous, and therefore, women who opt not to have them removed, should undergo regular monitoring and screening to ensure that they remain [benign](https://nabtahealth.com/glossary/benign/). Nabta is reshaping women’s healthcare. We support women with their personal health journeys, from everyday wellbeing to the uniquely female experiences of fertility, pregnancy, and [menopause](https://nabtahealth.com/glossary/menopause/). Get in [touch](/cdn-cgi/l/email-protection#5920383535381937383b2d38313c38352d31773a3634) if you have any questions about this article or any aspect of women’s health. We’re here for you. **Sources:** * Ben-Arie, Alon, et al. “The Malignant Potential of Endometrial [Polyps](https://nabtahealth.com/glossary/polyps/).” _European Journal of Obstetrics & Gynecology and Reproductive Biology_, vol. 115, no. 2, 10 Aug. 2004, pp. 206–210., doi:10.1016/j.ejogrb.2004.02.002. * Chan, Ssc, et al. “A Randomised Controlled Trial of [Prophylactic](https://nabtahealth.com/glossary/prophylactic/) Levonorgestrel Intrauterine System in Tamoxifen-Treated Women.” _BJOG: An International Journal of Obstetrics & Gynaecology_, vol. 114, no. 12, Dec. 2007, pp. 1510–1515., doi:10.1111/j.1471-0528.2007.01545.x. * Kanthi, Janu Mangala, et al. “Clinical Study of Endometrial Polyp and Role of Diagnostic Hysteroscopy and Blind Avulsion of Polyp.” _Journal Of Clinical And Diagnostic Research_, vol. 10, no. 6, June 2016, pp. QC01–4., doi:10.7860/jcdr/2016/18173.7983. * Nijkang, Njume Peter, et al. “Endometrial [Polyps](https://nabtahealth.com/glossary/polyps/): Pathogenesis, Sequelae and Treatment.” _SAGE Open Medicine_, vol. 7, 2 May 2019, doi:10.1177/2050312119848247. * Wong, M., et al. “The Natural History of Endometrial [Polyps](https://nabtahealth.com/glossary/polyps/).” _Human Reproduction_, vol. 32, no. 2, Feb. 2017, pp. 340–345., doi:10.1093/humrep/dew307.

You’re ready to start a family and you want to know what helps you get pregnant fast. Conceiving can take time, and fertility is different for every woman and couple. If you are trying for a baby, there are natural ways to increase your chances of getting pregnant. #### _Getting your body ready for pregnancy_ You can start by taking some lifestyle steps to prepare your body for conception. Your health before pregnancy can improve your chances of conceiving. And preconception wellbeing contributes to a healthy pregnancy. So, in the 3 to 4 months before trying for a baby: – Take **prenatal vitamins**: Start taking prenatal vitamins with [folic acid](https://nabtahealth.com/product/folic-acid-test/) before and during pregnancy to ensure your body is nutritionally strong, with all the [minerals and vitamins required for healthy fetal developmen](https://nabtahealth.com/articles/4-supplements-to-take-when-trying-to-conceive/)t. – Get a **well-woman health check**: Get a full preconception medical to flag any potential health issues that could affect you getting pregnant naturally or could affect your pregnancy. Use this check-up to make sure your vaccinations are up to date. – **Stop smoking, vaping,** and **drugs**. Limit **alcohol** intake and cut back on **caffeine**. – Eat a [**balanced diet**](https://nabtahealth.com/articles/eating-to-conceive/): Boost your health with a varied diet covering all five food groups. – Keep a **healthy weight**: Being underweight, obese or overweight can affect your fertility. – **Exercise** regularly: Exercise that builds strength, endurance and muscle tone will help your body stay healthy and strong during pregnancy and labour. – Get lots of sleep: Sleep patterns affect hormones. Stick to a regular 7-8 hours sleep routine as you prepare your body to conceive. – **Reduce stress**: High stress levels are linked with difficulties getting pregnant. – **Come off hormonal contraception**: If you’re on hormonal contraception (the pill, [IUD](https://nabtahealth.com/glossary/iud/), patch, ring implant) your body needs time to readjust and for cycles to return to your personal normal. #### _Know your fertile window_ Timing is everything when you want to conceive. You need to time sex with [ovulation](https://nabtahealth.com/glossary/ovulation/). The man’s [sperm](https://nabtahealth.com/glossary/sperm/) must meet and fertilise the woman’s egg at the right time. Knowing your fertile window and timing sexual intercourse with [ovulation](https://nabtahealth.com/glossary/ovulation/) is key to increasing your chances of getting pregnant. Women typically ovulate around 12 to 14 days before their next period. If your periods are regular (the average menstrual cycle is 28 days but it’s normal for women’s cycles to be anywhere from 21 to 40 days) you count back from the first day of when you would expect your next period. #### _Trying to get pregnant_ Have sex at least every 2 to 3 days in the [lead](https://nabtahealth.com/glossary/lead/)\-up to [ovulation](https://nabtahealth.com/glossary/ovulation/). [Sperm](https://nabtahealth.com/glossary/sperm/) can survive for several days in the female reproductive tract and once you’ve ovulated your egg has a 12-to-24-hour window for fertilisation, so for the best chances of conception have regular sex in the [lead](https://nabtahealth.com/glossary/lead/) up to that brief window. #### _What are the signs of [ovulation](https://nabtahealth.com/glossary/ovulation/)?_ Use fertility awareness methods to predict when you are most likely to conceive. If you have irregular cycles, combine these non-invasive physiological cues with tracking your menstrual cycle length to determine when you are most fertile: – Check [**cervical mucous**](https://www.mayoclinic.org/tests-procedures/cervical-mucus-method/about/pac-20393452): As you near [ovulation](https://nabtahealth.com/glossary/ovulation/) you’ll notice your discharge becomes clear, stretchy, and wet, with the consistency of raw egg whites. This means you are at your most fertile. – Chart your [**basal body temperature (BBT)**](https://my.clevelandclinic.org/health/treatments/21065-basal-body-temperature): There’s a small rise in body temperature after [ovulation](https://nabtahealth.com/glossary/ovulation/). Measuring BBT over 3-4 cycles will give a fairly accurate prediction of the exact point of [ovulation](https://nabtahealth.com/glossary/ovulation/). Other methods for tracking [ovulation](https://nabtahealth.com/glossary/ovulation/) include: – **Calendar method**: This works by recording menstrual cycles on a calendar for 6-12 months and calculating fertile periods. It’s most effective as a fertility predictor when combined with cervical mucous and BBT methods. – [](https://nabtahealth.com/articles/how-do-ovulation-predictor-kits-work/)**[Ovulation](https://nabtahealth.com/glossary/ovulation/) predictor kits**: Over the counter [ovulation](https://nabtahealth.com/glossary/ovulation/) kits work in a similar way to at-home pregnancy tests. You pee on a stick measuring luteinizing hormone and a surge in this hormone indicates [ovulation](https://nabtahealth.com/glossary/ovulation/). Unfortunately, this doesn’t prove an egg has been released and a woman can have the hormone surge but fail to ovulate. – **Period tracker apps**: Smartphone [ovulation](https://nabtahealth.com/glossary/ovulation/) tracker apps, like [OvuSense](https://nabtahealth.com/product/fertility-cycle-monitoring-with-ovusense/), monitor menstrual cycles and predict fertility. Fertility awareness, knowing and understanding your body and its menstrual cycles, and lots of patience, helps lots of couples to conceive. But getting pregnant isn’t always as straightforward as knowing your body and having lots of sex. If it’s taking longer than expected to fall pregnant, make an appointment with your healthcare team. If you are under 35 see a doctor after 12 months of trying for a baby. If you are over 35 seek advice after 6 months of trying to get pregnant. [Nabta Health](https://nabtahealth.com/) provides personalised and evidence-based support and resources for women, wherever they are on their fertility journey.

* Having ovarian cysts is not the same as being diagnosed with [](https://nabtahealth.com/articles/five-things-your-doctor-probably-wont-tell-you-about-pcos-polycystic-ovary-syndrom/)[PCOS](https://nabtahealth.com/glossary/pcos/). * Polycystic [ovaries](https://nabtahealth.com/glossary/ovaries/) syndrome is a condition caused by an excess in [androgens](https://nabtahealth.com/glossary/androgen/) (male hormones). * There are several different types of ovarian cysts which can cause [PCOS](https://nabtahealth.com/glossary/pcos/)\-like symptoms such as painful sex and irregular periods. * Only cysts that contain an egg (follicular) or did contain an egg (corpus luteum) are associated with polycystic [ovaries](https://nabtahealth.com/glossary/ovaries/) and [](https://nabtahealth.com/articles/five-things-your-doctor-probably-wont-tell-you-about-pcos-polycystic-ovary-syndrom/)[PCOS](https://nabtahealth.com/glossary/pcos/). The short answer is: no, ovarian cysts and [Polycystic Ovarian Syndrome (](https://nabtahealth.com/articles/five-things-your-doctor-probably-wont-tell-you-about-pcos-polycystic-ovary-syndrom/)[PCOS](https://nabtahealth.com/glossary/pcos/)) are definitely not the same thing. #### [PCOS](https://nabtahealth.com/glossary/pcos/) [PCOS](https://nabtahealth.com/glossary/pcos/) is a metabolic condition caused by an excess of androgen hormones that may or may not result in polycystic [ovaries](https://nabtahealth.com/glossary/ovaries/). Get your [blood tested for](https://nabtahealth.com/product/pcos-test/) [PCOS](https://nabtahealth.com/glossary/pcos/) in the privacy of your home. ### Polycystic [ovaries](https://nabtahealth.com/glossary/ovaries/) (PCO) To begin with, having [polycystic](../do-polycystic-ovaries-equal-pcos) [ovaries](https://nabtahealth.com/glossary/ovaries/) (PCO) is not the same thing as being diagnosed with [PCOS](https://nabtahealth.com/glossary/pcos/). Polycystic [ovaries](https://nabtahealth.com/glossary/ovaries/) contain a number of partially mature follicles. They are a normal variant of a woman’s ovary. But polycystic [ovaries](https://nabtahealth.com/glossary/ovaries/) are also not the same thing as ovarian cysts. When a woman has polycystic [ovaries](https://nabtahealth.com/glossary/ovaries/), the cysts referred to in “polycystic” (meaning “many cysts”) are known as **follicular cysts**. Follicular cysts form when a follicle containing an egg does not open and release the egg. The fluid inside the partially mature follicle then forms a cyst on the ovary. A follicular cyst is a type of **functional cyst**, meaning it serves some purpose within the ovary. The other type of functional cyst is a **corpus luteum**. After a follicle releases its egg, the follicle sac typically dissolves and is reabsorbed by the ovary. However, if the sac doesn’t dissolve and the opening of the follicle seals, additional fluid can develop inside the follicle creating a corpus luteum. #### Non-functional cysts Then there are **non-functional** cysts, or cysts that do not serve a purpose within the ovary. There are four types of non-functional cyst: * **Hemorrhagic cyst** – a hemorrhagic cyst occurs when there is bleeding into a follicular cyst or corpus luteum. Although these can be painful, most disappear spontaneously without follow-up. * **[Endometrioma](https://nabtahealth.com/glossary/endometrioma/)** – an [endometrioma](https://nabtahealth.com/glossary/endometrioma/) is a type of cyst that forms when endometrial tissue (the mucous membrane that makes up the inner layer of the uterine wall) grows inside the [ovaries](https://nabtahealth.com/glossary/ovaries/). * **Paraovarian cyst** – also known as a “paratubal” cyst, a paraovarian cyst is a fluid-filled sac that forms outside the [ovaries](https://nabtahealth.com/glossary/ovaries/) in the space around the [ovaries](https://nabtahealth.com/glossary/ovaries/) or [fallopian tubes](https://nabtahealth.com/glossary/fallopian-tube/). These cysts usually dissolve on their own and so are often undiagnosed. * **Teratoma** – a teratoma is a tumour made up of several types of tissue including hair, muscle or bone. Mature teratomas such as dermoid cysts are normally [benign](https://nabtahealth.com/glossary/benign/). Immature teratomas may be cancerous. Symptoms of Ovarian Cysts ------------------------- Symptoms of ovarian cysts can include: * Abdominal pain, especially during intercourse * Pain during or shortly after the beginning or end of your period * Irregular periods, or abnormal uterine bleeding or spotting. * Fullness, heaviness, pressure, swelling, or bloating in the abdomen. * Change in frequency or ease of urination * Difficulty with bowel movements due to pressure on the pelvis * Fatigue and headaches * Nausea or vomiting * Weight gain When cysts rupture or burst, and this can happen to functional and non-functional cysts as both contain fluid, you may experience a sudden and sharp pain in the lower abdomen on one side. Usually there are no further complications, although if a particularly large cyst ruptures it can cause internal bleeding. If you are worried, consult your doctor. Conclusion ---------- If you are diagnosed with “ovarian cysts”, it is important that you clarify exactly what type of ovarian cysts you have. Remember that only functional cysts – follicular cysts and corpus luteum – are related to PCO or [PCOS](https://nabtahealth.com/glossary/pcos/). Nabta is reshaping women’s healthcare. We support women with their personal health journeys, from everyday wellbeing to the uniquely female experiences of fertility, pregnancy, and [menopause](https://nabtahealth.com/glossary/menopause/). Get in [touch](/cdn-cgi/l/email-protection#aed7cfc2c2cfeec0cfccdacfc6cbcfc2dac680cdc1c3) if you have any questions about this article or any aspect of women’s health. We’re here for you. **Sources** * “Ovarian cysts”. Office on Women’s Health. November 19, 2014. Archived from the original on 29 June 2015. Retrieved 27 June 2015. * Hemorrhagic ovarian cysts: Clinical and sonographic correlation with the management options, Ahmed M.Abbasa, Mariam T.Aminb, Sara M.Tolbac, Mohamed K.Alia, https://doi.org/10.1016/j.mefs.2015.08.001 * “Mature teratoma”. National Cancer Institute. Retrieved 20 December 2017. * Noor, Mohd Rushdan Md; Hseon, Tay Eng; Jeffrey, Low Jen Hui (2014). Gynaecologic Cancer: A Handbook for Students and Practitioners. CRC Press. p. 446. ISBN 9789814463065.

 Deciding you want to become pregnant and have a baby can be an incredibly exciting and overwhelming time. Fertility can be affected by many factors and there are ways to increase your chances of conceiving naturally. However, for some trying for a baby may not go as hoped or planned, and they might need further medical assistance to conceive. Wherever you are on your fertility journey, [Nabta Health](https://nabtahealth.com/shop/collections/stage/fertility/) will support you with resources, knowledge, and access to experts. #### How can I increase my chances of getting pregnant naturally? First things first. There are lifestyle steps you can take in the months before you start trying for a baby to prepare your body for conception. * Take **prenatal vitamins**: To ensure your body is nutritionally strong, with all the minerals and vitamins you need for strong fetal development, start taking prenatal vitamins with folic acid at least three months before you try to conceive. * Follow a **balanced diet**: Boost your health with a varied diet covering all food groups. Avoid refined sugars, saturated fats and too much salt. * Maintain a **healthy weight**: Being underweight or overweight can impact fertility. * **Exercise** regularly: Exercise that builds strength, endurance and muscle tone will help your body stay healthy and strong during pregnancy and labour. * Get lots of **rest** and **sleep**: Sleep patterns can affect hormones. Stick to a regular 7-8 hours sleep routine as you prepare your body to conceive. * **Reduce stress**: High stress levels are linked with difficulties getting pregnant. Give yourself a break when you can and take the pressure off. If you’re feeling frazzled, try taking up yoga and practice mindfulness. * **Stop smoking** and **quit drugs**. Limit **alcohol** intake and cut back on **caffeine**. * **Come off contraception**: If you’re on hormonal contraception (the pill, [IUD](https://nabtahealth.com/glossary/iud/), patch, ring implant) it can take some months for your body to readjust and your cycles to return to your personal ‘normal’. Of course, this doesn’t apply if you use condoms or a diaphragm for contraception as they simply act as a barrier to conceiving. * Get a **well-woman health check**: Consider getting a full medical, including a check-up for any sexually transmitted infections (STIs). While this is by no means essential, your healthcare team will help you manage any potential red flags, family medical history or underlying health conditions that could af you getting pregnant naturally or having a healthy pregnancy. #### How do women become pregnant? The traditional way for heterosexual couples to get pregnant is through unprotected sexual intercourse. Pregnancy is a question of timing (among other individual factors). Heterosexual couples who want to get pregnant will need to time sex with [ovulation](https://nabtahealth.com/glossary/ovulation/). The man’s [sperm](https://nabtahealth.com/glossary/sperm/) must meet and fertilise the egg at the right time. Knowing her fertile window and timing intercourse with [ovulation](https://nabtahealth.com/glossary/ovulation/) is one of the most important factors in increasing a woman’s chances of conceiving. #### What is [ovulation](https://nabtahealth.com/glossary/ovulation/)? The [ovaries](https://nabtahealth.com/glossary/ovaries/) release the egg once every cycle, during [ovulation](https://nabtahealth.com/glossary/ovulation/). That egg travels down the [fallopian tubes](https://nabtahealth.com/glossary/fallopian-tube/) and waits to be fertilised by a [sperm](https://nabtahealth.com/glossary/sperm/). The egg can wait for 12-24 hours for a [sperm](https://nabtahealth.com/glossary/sperm/) to successfully push through its outer surface. [Sperm](https://nabtahealth.com/glossary/sperm/) can live inside the female reproductive tract for 3-5 days waiting to fertilise an egg. All being good the fertilised egg makes its way to the [uterus](https://nabtahealth.com/glossary/uterus/) (womb) and implants in the uterine lining. #### How do I know when I’m ovulating? Women typically ovulate around 12 to 14 days before their next period. If you have regular periods (the average menstrual cycle is 28 days but it’s normal for women’s cycles to be anywhere from 21 to 40 days) you can count back from the first day of when you would expect your next period. Fertility experts recommend having sex at least every other day in the [lead](https://nabtahealth.com/glossary/lead/)\-up to [ovulation](https://nabtahealth.com/glossary/ovulation/). [Sperm](https://nabtahealth.com/glossary/sperm/) can survive for several days in the female reproductive tract but once you’ve ovulated your egg has a 12-24 window for fertilisation so for the best chances of conception have enough sex in the time leading up to that brief window. #### What is fertility awareness and natural family planning? Fertility awareness methods (FAMs), also known as natural family planning, is used by women both as a method of contraception and to predict when they are most likely to conceive. Women can monitor several physiological cues alongside tracking menstrual cycle length to determine when they are most fertile: * Checking **cervical mucous**: Understanding how your cervical mucous changes during your cycle. As you near [ovulation](https://nabtahealth.com/glossary/ovulation/) you’ll notice your discharge becomes clear, stretchy, and wet, with the consistency of raw egg whites. This is known as fertile quality mucous and you are now at your most fertile. * Charting your **basal body temperature (BBT)**: There is a small rise in body temperature after [ovulation](https://nabtahealth.com/glossary/ovulation/). Measuring your BBT can help you predict the exact point of [ovulation](https://nabtahealth.com/glossary/ovulation/). Women with regular periods can measure BBT for 3-4 cycles to gain a fairly accurate prediction of when they are most fertile * Monitoring cervical mucous and BBT are non-invasive, easily accessible methods to track fertility. Using these two approaches together is known as the symptothermal method. Other methods for tracking [ovulation](https://nabtahealth.com/glossary/ovulation/) include: * **Calendar method**: This works by recording menstrual cycles on a calendar for 6-12 months and calculating fertile periods. It is most effective as a fertility predictor when combined with cervical mucous and BBT methods. * **[Ovulation](https://nabtahealth.com/glossary/ovulation/) predictor kits**: Over the counter [ovulation](https://nabtahealth.com/glossary/ovulation/) kits work in a similar way to at-home pregnancy tests. The woman pees on a stick measuring luteinizing hormone and a surge in this hormone indicates [ovulation](https://nabtahealth.com/glossary/ovulation/). However, it doesn’t prove an egg has been released and a woman can have the hormone surge but fail to ovulate. * **Period tracker apps**: Smartphone [ovulation](https://nabtahealth.com/glossary/ovulation/) tracker apps, like [OvuSense](https://nabtahealth.com/product/fertility-cycle-monitoring-with-ovusense/), monitor menstrual cycles and predict fertility. If you do choose to use a smartphone tracker app, be sure to read the small print for data collection policies. Fertility awareness, knowing and understanding your body and its menstrual cycles, helps lots of couples to conceive. However, getting pregnant isn’t always as simple as knowing your body and having lots of ‘baby making sex’. Some women want children but either cannot conceive naturally or keep miscarrying. And obviously, there are different considerations for women who have irregular periods due to [endometriosis](https://nabtahealth.com/glossary/endometriosis/) or [PCOS](https://nabtahealth.com/glossary/pcos/), those whose fertility is affected by illness or genetic history, and people who are single, transgender, or in same-sex relationships. #### What affects female fertility? Egg numbers and quality start to decline after 35, increasing the risk of age-related [infertility](https://nabtahealth.com/glossary/infertility/). The risk of pregnancy-related complications also increases with age. Underlying health issues, [endometriosis](https://nabtahealth.com/glossary/endometriosis/), uterine [polyps](https://nabtahealth.com/glossary/polyps/) or [fibroids](https://nabtahealth.com/glossary/fibroids/), polycystic ovarian syndrome ([PCOS](https://nabtahealth.com/glossary/pcos/)), problems with the [fallopian tubes](https://nabtahealth.com/glossary/fallopian-tube/), and ovulatory problems can all affect fertility. #### What affects male fertility? Male fertility problems can be caused by low [sperm](https://nabtahealth.com/glossary/sperm/) count, poor quality [sperm](https://nabtahealth.com/glossary/sperm/), or blockages preventing [sperm](https://nabtahealth.com/glossary/sperm/) moving through the reproductive tract. [Sperm](https://nabtahealth.com/glossary/sperm/) can be vulnerable to lifestyle and environmental factors including raised body temperature, weight gain, exposure to toxins, smoking, heavy alcohol intake and drug use. #### What if I can’t get pregnant naturally? Doctors define [infertility](https://nabtahealth.com/glossary/infertility/) as the inability to conceive after one year or longer of regular unprotected sex. If you are a woman in a heterosexual relationship and struggling to conceive using fertility awareness and natural family planning methods, both you and your partner should seek a medical and physical evaluation. In some situations, if a woman is 35 years or older, doctors may decide to investigate and treat [infertility](https://nabtahealth.com/glossary/infertility/) after 6 months of unprotected intercourse. #### Fertility testing for women Testing will depend on individual health and medical history, but typically initial testing will include **routine blood work to** check for: * Anti-Müllerian Hormone ([AMH](https://nabtahealth.com/glossary/amh/)): Ovarian reserve test to estimate how many eggs a woman has. * Follicle-Stimulating Hormone ([FSH](https://nabtahealth.com/glossary/fsh/)): Hormone stimulates the follicle producing the eggs. * Luteinizing Hormone ([LH](https://nabtahealth.com/glossary/lh/)): Responsible for follicle production and egg maturation. * [Prolactin](https://nabtahealth.com/glossary/prolactin/) (PRL): Hormone released from anterior pituitary gland, raised during pregnancy in preparation for breastfeeding, and in women with infrequent periods. * Thyrotrophin ([TSH](https://nabtahealth.com/glossary/tsh/)): Can indicate an underactive thyroid, linked with irregular periods. * [Estradiol](https://nabtahealth.com/glossary/estradiol/): A form of estrogen, the test measures ovarian function and egg quality. * Androgen: High levels can prevent the [ovaries](https://nabtahealth.com/glossary/ovaries/) from releasing an egg and may indicate polycystic ovarian syndrome ([PCOS](https://nabtahealth.com/glossary/pcos/)). * A **Vaginal ultrasound** will check: 1. Reproductive organ health. 2. [Ovaries](https://nabtahealth.com/glossary/ovaries/) for cysts, [fibroids](https://nabtahealth.com/glossary/fibroids/), [polyps](https://nabtahealth.com/glossary/polyps/), [PCOS](https://nabtahealth.com/glossary/pcos/), [endometriosis](https://nabtahealth.com/glossary/endometriosis/), or any abnormalities. 3. Egg reserve. Sometimes an **X-ray** is also carried out: Hysterosalpingography (HSG): Examines inside of the [uterus](https://nabtahealth.com/glossary/uterus/) (womb) and [fallopian tubes](https://nabtahealth.com/glossary/fallopian-tube/) for blockages or anything that might be stopping the [sperm](https://nabtahealth.com/glossary/sperm/) from reaching the egg. #### Fertility testing for men Blood work for men will check hormone levels and scan for certain infections or a possible genetic cause for [infertility](https://nabtahealth.com/glossary/infertility/). A doctor may request a [sperm](https://nabtahealth.com/glossary/sperm/) sample to assess [sperm](https://nabtahealth.com/glossary/sperm/) count, shape and movement, and a scrotal ultrasound to check if there are any problems or blockages in the testicles preventing [sperm](https://nabtahealth.com/glossary/sperm/) getting into a man’s ejaculate. #### Fertility treatment options Each person’s fertility scenario is unique, and any recommended [infertility](https://nabtahealth.com/glossary/infertility/) treatment will depend on an individual’s own health and medical history. A woman with a blocked fallopian tube or a man who isn’t producing [sperm](https://nabtahealth.com/glossary/sperm/) will be offered procedures to remove the blockage, repair damage or retrieve [sperm](https://nabtahealth.com/glossary/sperm/), before trying other fertility treatments. If appropriate, fertility specialists will often recommend that women start with **clomid**, a **prescribed oral medication for [infertility](https://nabtahealth.com/glossary/infertility/)**. This is also the preferred approach for women with hormonal conditions such as polycystic ovarian syndrome ([PCOS](https://nabtahealth.com/glossary/pcos/)). Clomid works by stimulating an increase in the levels of follicle-stimulating hormones, initiating [ovulation](https://nabtahealth.com/glossary/ovulation/) and increasing the odds of pregnancy. For some women this approach is combined with **intrauterine insemination (IUI)**, in which the male partner’s or donor’s [sperm](https://nabtahealth.com/glossary/sperm/) is inserted directly into the [uterus](https://nabtahealth.com/glossary/uterus/) to increase the probabilities of conception. If that approach doesn’t work, or if it’s clear from a woman’s medical history it won’t work, the next step would be treatments such as **in vitro fertilisation ([IVF](https://nabtahealth.com/glossary/ivf/))**. [IVF](https://nabtahealth.com/glossary/ivf/) involves retrieving eggs from a woman’s body, fertilising the eggs in a laboratory, and transferring the resulting embryo back into her body. The process is lengthy, invasive, and expensive and can take an emotional toll. However, for many women who want children it is their only option. Fertility treatments vary depending on a woman or couple’s situation. People who are single, in same-sex relationships or transgender will have their own fertility journeys and in these cases a woman’s age and fertility status still plays a role. Fertility experts will offer the necessary support and advice for each individual scenario. #### Getting started on your fertility journey with Nabta Health Whatever your personal situation, whether you’re thinking about starting a family, having another child, or you’ve been trying for years without success, [Nabta Health](https://nabtahealth.com/shop/collections/stage/fertility/) will support you on your fertility journey. From health and lifestyle tips for pre-conception and [PCOS](https://nabtahealth.com/glossary/pcos/), to relationship coaching, pregnancy wellness products, and at-home vitamin, thyroid, and fertility testing, Nabta’s fertility marketplace and knowledge resources are designed to accompany you through each stage from pre-conception to birth.

#### **What is [Sperm](https://nabtahealth.com/glossary/sperm/)?** [Sperm](https://nabtahealth.com/glossary/sperm/) is the male reproductive cell. It is produced in the testes from [germ cells](https://nabtahealth.com/glossary/germ-cells/). Upon reaching [puberty](https://nabtahealth.com/glossary/puberty/), a man produces millions of [sperm](https://nabtahealth.com/glossary/sperm/) every day. A [sperm](https://nabtahealth.com/glossary/sperm/) is very small, about 0.05 mm long. A mature [sperm](https://nabtahealth.com/glossary/sperm/) cell contains a head and a short tail. This head has the genetic material of the male. The [sperm](https://nabtahealth.com/glossary/sperm/) is a haploid, which means it contains only 23 [chromosomes](https://nabtahealth.com/glossary/chromosomes/), unlike the 46 [chromosomes](https://nabtahealth.com/glossary/chromosomes/) found in other cells of the body. This is because during fertilisation, the semen fuses with the egg, the woman’s reproductive cell, which is also haploid, to form a [zygote](https://nabtahealth.com/glossary/zygote/) which has 46 [chromosomes](https://nabtahealth.com/glossary/chromosomes/). The [zygote](https://nabtahealth.com/glossary/zygote/) later implants itself in the [uterus](https://nabtahealth.com/glossary/uterus/) of the female, becomes the embryo which, if all is well, will develop into a baby. The process of a germ cell in the testes developing into a fully mature semen cell, capable of fertilising an egg, involves a number of steps and the whole process takes about 2.5 months. #### **Production of [sperm](https://nabtahealth.com/glossary/sperm/) and semen** The testes have a system of tiny tubes called [seminiferous tubules](https://nabtahealth.com/glossary/seminiferous-tubules/). These tubes contain simple round [germ cells](https://nabtahealth.com/glossary/germ-cells/) at birth. Once the male reaches [puberty](https://nabtahealth.com/glossary/puberty/), [testosterone](https://nabtahealth.com/glossary/testosterone/) (the principle male sex hormone), in combination with other hormones, known as [androgens](https://nabtahealth.com/glossary/androgen/), stimulates the development of the [germ cells](https://nabtahealth.com/glossary/germ-cells/) into [sperm](https://nabtahealth.com/glossary/sperm/) cells. Once developed, the [sperm](https://nabtahealth.com/glossary/sperm/) cells move, first into the [epididymis](https://nabtahealth.com/glossary/epididymis/), and then 5 weeks later, into the [vas deferens](https://nabtahealth.com/glossary/vas-deferens/), which is also known as the [sperm](https://nabtahealth.com/glossary/sperm/) duct. The [sperm](https://nabtahealth.com/glossary/sperm/) cells mix with seminal fluid from the seminal vesicles and prostate gland to form semen. The semen is what enters the female body to fuse with the egg for fertilisation when ejaculated. The seminal fluid promotes the survival of the [sperm](https://nabtahealth.com/glossary/sperm/) cells in the female [uterus](https://nabtahealth.com/glossary/uterus/) and provides nutrition to the milt. #### **Impact of [sperm](https://nabtahealth.com/glossary/sperm/) on fertility** Males are [solely responsible](../who-is-responsible-for-infertility) for about 20 – 30% of [infertility](https://nabtahealth.com/glossary/infertility/) cases. There are many factors that can affect the [health of a male’s](../causes-of-male-infertility) [sperm](https://nabtahealth.com/glossary/sperm/), including genetics, [the environment](../environmental-factors-that-contribute-to-male-infertility), hormonal issues, poor semen quality, and structural abnormalities of the male reproductive system. It is important for a male to maintain [sperm](https://nabtahealth.com/glossary/sperm/) health if he is planning to conceive, as [sperm](https://nabtahealth.com/glossary/sperm/) quality not only affects the likelihood of successful conception, but also influences the outcome of pregnancy; with abnormal [chromosomes](https://nabtahealth.com/glossary/chromosomes/),[sperm](https://nabtahealth.com/glossary/sperm/) DNA fragmentation and even lifestyle choices having the potential to affect the viability and health of offspring. #### **Maintaining the health of a male’s [sperm](https://nabtahealth.com/glossary/sperm/)** Measures of [sperm](https://nabtahealth.com/glossary/sperm/) health include [sperm](https://nabtahealth.com/glossary/sperm/) count, [sperm](https://nabtahealth.com/glossary/sperm/) strength and [how well it moves](../low-sperm-motility-asthenozoospermia). Healthy [sperm](https://nabtahealth.com/glossary/sperm/) have a well-rounded head and a strong tail that can help them swim fast. A [healthy](../my-husband-has-a-low-sperm-count-when-is-the-best-time-during-the-menstrual-cycle-to-have-intercourse) [sperm](https://nabtahealth.com/glossary/sperm/) count is about 15 million or more for every milliliter (mL) of semen. Having a high [sperm](https://nabtahealth.com/glossary/sperm/) count increases the chances of one of them making it through the female reproductive system and fertilising an egg. Maintaining [sperm](https://nabtahealth.com/glossary/sperm/) health is important for the individual and for future generations. Here are some lifestyle approaches that can help to keep spunk healthy & strong, and to improve fertility: * Eat well and maintain a [healthy diet](../do-vitamins-and-other-nutritional-products-improve-sperm-count) * Avoid smoking or using illicit drugs * Limit alcohol and caffeine intake * Keep the scrotum cool by avoiding tight trousers * Exercise regularly but not intensely * Try to minimise exposure to pesticides and heavy metals * Minimise physical and emotional stress * Make sure to get enough [zinc](https://nabtahealth.com/glossary/zinc/) and other essential vitamins It can be stressing sometimes not sure what is wrong try Nabta’s [men’s health test](https://nabtahealth.com/product/mens-health-test/) and get to learn more. Nabta is reshaping women’s healthcare. We support women with their personal health journeys, from everyday wellbeing to the uniquely female experiences of fertility, pregnancy, and [menopause](https://nabtahealth.com/glossary/menopause/). Get in [touch](/cdn-cgi/l/email-protection#3d445c51515c7d535c5f495c55585c514955135e5250) if you have any questions about this article or any aspect of women’s health. We’re here for you. **Sources:** * Akmal, M., et al. (2006). Improvement in Human Semen Quality After Oral Supplementation of Vitamin C. _Journal of Medicinal Food_, 9(3), pp.440-442. * Blomberg Jensen, M., et al. (2011). [Vitamin D](https://nabtahealth.com/glossary/vitamin-d/) is positively associated with semen [motility](https://nabtahealth.com/glossary/motility/) and increases intracellular calcium in human spermatozoa. _Human Reproduction_, 26(6), pp.1307-1317. * Colagar, A., et al. (2009). [Zinc](https://nabtahealth.com/glossary/zinc/) levels in seminal plasma are associated with semen quality in fertile and infertile men. _Nutrition Research_, 29(2), pp.82-88. * Danielewicz, A., et al. (2018). Dietary Patterns and Poor Semen Quality Risk in Men: A Cross-Sectional Study. _Nutrients_, 10(9), p.1162. * Fullston, T., et al. (2017). The most common vices of men can damage fertility and the health of the next generation. _Journal of Endocrinology_, 234(2), F1-F6. doi: 10.1530/joe-16-0382. * “Male [Infertility](https://nabtahealth.com/glossary/infertility/) – Symptoms And Causes”. _Mayo Clinic_, 2019, [https://www.mayoclinic.org/diseases-conditions/male-](https://www.mayoclinic.org/diseases-conditions/male-infertility/symptoms-causes/syc-20374773)[infertility](https://nabtahealth.com/glossary/infertility/)/symptoms-causes/syc-20374773. * “Male Reproductive System (For Parents) – Kidshealth”. _Kidshealth.Org_, 2019, [https://kidshealth.org/en/parents/male-reproductive.html](https://kidshealth.org/en/parents/male-reproductive.html). * Janevic, T., et al. (2014). Effects of work and life stress on semen quality. _Fertility and Sterility_, 102(2), pp.530-538. * Jensen, T., et al. (2014). Habitual alcohol consumption associated with reduced semen quality and changes in reproductive hormones; a cross-sectional study among 1221 young Danish men. _BMJ Open_, 4(9), pp.e005462-e005462. * Jouannet, Pierre et al. “Semen Quality And Male Reproductive Health: The Controversy About Human milt Concentration Decline”. _APMIS_, vol 109, no. S103, 2001, pp. S48-S61. Wiley, doi:10.1111/j.1600-0463.2001.tb05801.x. * Jóźków, P. and Rossato, M. (2016). The Impact of Intense Exercise on Semen Quality. _American Journal of Men’s Health_, 11(3), pp.654-662. * Vaamonde, D., et al. (2012). Physically active men show better semen parameters and hormone values than sedentary men. _European Journal of Applied Physiology_, 112(9), pp.3267-3273.

We have done the research for you and compiled the top 10 polycystic ovary syndrome ([PCOS](https://nabtahealth.com/glossary/pcos/)) doctors in Dubai, based on real patient experience and feedback. Based on recommendations from users on social media forums and direct [community feedback](/cdn-cgi/l/email-protection#2851494444496846494a5c49404d49445c40064b4745) to the Nabta Team, these recommended consultants are all well-known for their clinical expertise amongst UAE residents of a diverse range of cultures and backgrounds. #### Dr Marlain Mubarak, Consultant [Obstetrician](https://nabtahealth.com/glossary/obstetrician/) & [Gynaecologist](https://nabtahealth.com/glossary/gynaecologist/) [King’s College Hospital Dubai](https://kingscollegehospitaldubai.com/dr/marlain-mubarak/) Dr Marlain has been treating patients in Dubai since 2018 and is now at King’s College Hospital in Jumeirah. Her particular area of expertise is [endometriosis](https://nabtahealth.com/glossary/endometriosis/) and [PCOS](https://nabtahealth.com/glossary/pcos/).She was trained at the Oxford Deanery, UK and awarded by the Royal College of [obstetrician](https://nabtahealth.com/glossary/obstetrician/) and [Gynaecologist](https://nabtahealth.com/glossary/gynaecologist/) CCT in 2005 to become a consultant OBGyn. Dr Marlain has continued her work in improving outcomes for [endometriosis](https://nabtahealth.com/glossary/endometriosis/) patients in Dubai, by establishing a BSGE advanced [](https://kingscollegehospitaldubai.com/service/gynaecology-clinic/specific-gynaecological-disorders/endometriosis/endometriosis-centre/)[endometriosis](https://nabtahealth.com/glossary/endometriosis/) centre in King’s College Hospital Dubai which she leads. In 2019 she was awarded the UAE Healthcare award of best physician for contribution to health care and education. Dr Marlain is very well thought-of by her patients who call her “incredible”, “she cares about details, takes her time to investigate before any procedure”. #### ****Dr. Janeta Atanassova, MD**, Specialist Gynecologist, [Well Woman Clinic](https://www.wellwomanclinic.ae/our-physicians)** Dr Janeta has worked in Dubai for over 13 years, at Infinity Clinic and now at Well Woman Clinic. She has a very loyal following of patients who praise her for her experience in diagnosing and managing [PCOS](https://nabtahealth.com/glossary/pcos/). Dr. Janeta is an expert in gynecological and obstetric ultrasound and is highly skilled at diagnosing uterine and ovarian abnormalities. She also performs colposcopy examinations and treatments. Dr. Janeta uses minimally invasive surgical techniques such as [laparoscopy](https://nabtahealth.com/glossary/laparoscopy/) and hysteroscopy. Originally an academic in Obstetrics and Gynaecology at the University Hospital in Sofia, Dr Janeta completed her medical training in the UK, the Netherlands and in the USA. Well known for being direct and matter of fact, women have been relying on Dr Janeta for over 12 years and her patients have described her as “amazing”. #### **Dr. Leila Soudah, **Consultant [Obstetrician](https://nabtahealth.com/glossary/obstetrician/) and [Gynaecologist](https://nabtahealth.com/glossary/gynaecologist/)**, [DLS Clinic](https://dlsclinic.com/dr-leila-soudah.php)** With more than 21 years of experience in Dubai and 20 years in Germany, Dr Leila has run her own clinic, the Dr Leila Soudah clinic, since 1998. She is a passionate supporter of holistic care for women and has launched weight loss programs, along with a focus on anti-aging and regenerative medicine. Dr Leila has helped countless women with [PCOS](https://nabtahealth.com/glossary/pcos/) reduce their symptoms and conceive. Dr. Leila Soudah is a German Board certified Specialist in Obstetrics and Gynecology. She received her Doctor of Medicine in Berlin University and completed her Post graduation in Hannover University, Germany. In December 2015, she achieved post-graduation as Fellow in Metabolic and Nutrition Medicine in Las Vegas, USA. Her patients describe her as “an amazing doctor”. #### **Dr. Salma Ballal, Consultant [Obstetrician](https://nabtahealth.com/glossary/obstetrician/) and [Gynaecologist](https://nabtahealth.com/glossary/gynaecologist/),** [Genesis Healthcare Center](https://www.genesis-dubai.com/our_doctors/dr-salma-ballal/) Dr Salma is a popular OBGYN and has gathered a following of ‘raving fans’ who praise her care and bedside manner. Her [PCOS](https://nabtahealth.com/glossary/pcos/) expertise focuses on helping women overcome their symptoms to be able to successful conceive. Along with her expertise in managing [PCOS](https://nabtahealth.com/glossary/pcos/), Dr Salma manages a wide range of gynaecological conditions such as menstrual disturbances, [menopause](https://nabtahealth.com/glossary/menopause/) disorders, sexual dysfunction, vaginal rejuvenation, family planning and cervical pathology screening. Dr Salma trained as a Consultant [Obstetrician](https://nabtahealth.com/glossary/obstetrician/) and [Gynaecologist](https://nabtahealth.com/glossary/gynaecologist/) with the NHS developing a particular interest in maternal medicine, high-risk pregnancies and labour care.has completed the Royal College of [Obstetrician](https://nabtahealth.com/glossary/obstetrician/) and [Gynaecologist](https://nabtahealth.com/glossary/gynaecologist/) advanced training modules in maternal medicine and advanced labour ward practice. Patient social media feedback on Dr Salma said her patience guidance was “gentle and confident”. #### **Dr Elsa De Menezes Fernandes, **Consultant [Obstetrician](https://nabtahealth.com/glossary/obstetrician/) and [Gynaecologist](https://nabtahealth.com/glossary/gynaecologist/)**, [New Concept Clinic](https://drelsa.net/)** With almost 30 years’ experience, Dr Elsa was a very popular OBGYN at City Hospital for 7 years before starting up her own clinic, the Dr Elsa New Concept Clinic. Dr Elsa is “well liked by both her peers and patients and offers a personalised and patient centred care”. Dr Elsa diagnoses and treats [PCOS](https://nabtahealth.com/glossary/pcos/), recommending the best option for women with polycystic ovarian syndrome symptoms, including surgery where necessary. Dr Elsa de Menezes Fernandes is a UK trained [Obstetrician](https://nabtahealth.com/glossary/obstetrician/) and [Gynaecologist](https://nabtahealth.com/glossary/gynaecologist/). She completed her basic training in Goa, India, graduating from Goa University in 1993. Patients of Dr Elsa say she is “highly recommended” and describe her as “beyond amazing”. #### **Dr. Amal Alias**, ****Consultant [Obstetrician](https://nabtahealth.com/glossary/obstetrician/) and [Gynaecologist](https://nabtahealth.com/glossary/gynaecologist/)**,** [Dr Amal Alias Fertility and Gynaecology Center](https://a-ivf.ae/) Dr Amal is a specialist in gyncaecological diagnosis including [pelvic examination](https://nabtahealth.com/glossary/pelvic-examination/) as an important step to ensure a gynecological wellbeing. Focusing on menstrual irregularities and [PCOS](https://nabtahealth.com/glossary/pcos/), Dr Amal helps couples overcome fertility issues. Dr. Amal has more than two decades of experience in the UAE, working in a renowned Ministry of Health approved hospital as Specialist OBGYN and running her own clinic for more than two decades, at Dr. Amal Alias Gynaecology and Obstetrics Clinic Karama / JLT and Dr. Amal Alias Fertility & Gynaecology Center. Dr Amal graduateed from The Schenov First Moscow Medical University in 1988 and completed the Obs/Gynecological post graduate program in 1993. She is an active member of British Fertility Society. Dr Amal’s patients describe her as “simply the best and the easiest person to talk to”. #### **Dr Munira Furniturewala, Specialist [Gynaecologist](https://nabtahealth.com/glossary/gynaecologist/) and [Obstetrician](https://nabtahealth.com/glossary/obstetrician/) with subspecialty in Reproductive Endocrinology and [Infertility](https://nabtahealth.com/glossary/infertility/)**, [Mediclinic City Hospital](https://www.mediclinic.ae/en/corporate/doctors/7/munira-furniturewala-dr.html) Dr Munira has over 22 years’ experience in women’s health. Dr Munira has supported women through their diagnosis and treatment of [PCOS](https://nabtahealth.com/glossary/pcos/). During the last 15 years she has specialized in Fertility Management and is experienced in providing comprehensive fertility workup and management of couples seeking conception, including advanced assisted reproductive technologies. Dr. Munira’s professional interests include assisted reproductive treatments, Ultrasound guided operations , Colposcopy Hysteroscopy and Obstetric & Gynaec ultrasounds. Patient feedback on Dr Samina is overwhelmingly positive, describing her as “wonderful”, “absolutely fantastic”, “caring” and “amazing”. #### **Dr Vibha Sharma, Specialist [Gynaecologist](https://nabtahealth.com/glossary/gynaecologist/),** [**Prime Medical Center**](https://www.primehealth.ae/prime-medical-centers/medical-centers/prime-medical-center-sheikh-zayed-road/dr-vibha-sharma) Working in Dubai since 2004, Dr Vibha is known for her commitment to supporting women with a range of gynaecological and women’s health problems, including [PCOS](https://nabtahealth.com/glossary/pcos/). In the UAE she worked at Ministry of Health and Tertiary Care hospitals prior to joining Prime Medical Center. Dr Vibha specialises in areas of women’s health requiring specialist gynaecological expertise and is well-known for supporting women with [PCOS](https://nabtahealth.com/glossary/pcos/). Qualified in India at Jammu Medical College, Dr Vibha went on to do her post-graduate at King George’s Medical College in Lucknow. She worked at Queen Mary’s Hospital Lucknow and Willingdon and Batra Hospitals and Research Centre in New Delhi before moving to the Middle East. Patients have described Dr Vibha as “consistent”, “approachable”, and “professional”. #### Dr Samina Dornan, Consultant [Obstetrician](https://nabtahealth.com/glossary/obstetrician/) and [Gynaecologist](https://nabtahealth.com/glossary/gynaecologist/), Sub-specialist Maternal Fetal Medicine, [King’s College Hospital](https://kingscollegehospitaldubai.com/dr/samina-m-dornan/) Well known for her expertise in managing high risk mothers, their pregnancies and fetuses, Dr Samina is also a highly experienced gynaecological doctor, and supports women with [PCOS](https://nabtahealth.com/glossary/pcos/) through conception and pregnancy. Dr Samina is the first female Maternal Fetal Medicine sub Specialist, from the Royal College of [Obstetrician](https://nabtahealth.com/glossary/obstetrician/) and [Gynaecologist](https://nabtahealth.com/glossary/gynaecologist/), London to be here in Dubai. Her areas of expertise include: prenatal counseling, Fetal Growth Restriction, prenatal diagnosis and fetal therapy, fetal genetic disorders, including trisomies and fetal structural abnormalities including congenital diaphragmatic hernia. Dr Samina has an MD degree from Queen’s University Belfast, UK, and was Consultant [Obstetrician](https://nabtahealth.com/glossary/obstetrician/) [Gynaecologist](https://nabtahealth.com/glossary/gynaecologist/) at the Royal Maternity Hospital Belfast, Belfast Trust, UK. In 2017 she received a Fellowship from the Royal College of Obstetricians and Gynecologists, London. Patients say they “can’t recommend Dr Samina highly enough”. \_\_\_ If you are concerned you may have [PCOS](https://nabtahealth.com/glossary/pcos/), get tested in the privacy of your own home by ordering a [PCOS](https://nabtahealth.com/glossary/pcos/) blood test [here.](https://nabtahealth.com/product/pcos-test/) Nabta is reshaping women’s healthcare. We support women with their personal health journeys, from everyday wellbeing to the uniquely female experiences of fertility, pregnancy, and [](https://nabtahealth.com/glossary)[menopause](https://nabtahealth.com/glossary/menopause/). You can track your menstrual cycle and get [personalised support by using the Nabta app.](https://nabtahealth.com/our-platform/nabta-app/) [Get in touch](/cdn-cgi/l/email-protection#1c392e2c657d70707d5c727d7e687d74797d706874327f7371) if you have any questions about this article or any aspect of women’s health. We’re here for you. _Updated June 2022_ If you would like to recommend a doctor, we’d love to hear from you: we rely on our community to give us their reviews so we can pass on to our readers. Please contact [\[email protected\]](/cdn-cgi/l/email-protection#dfa6beb3b3be9fb1bebdabbeb7babeb3abb7f1bcb0b2)
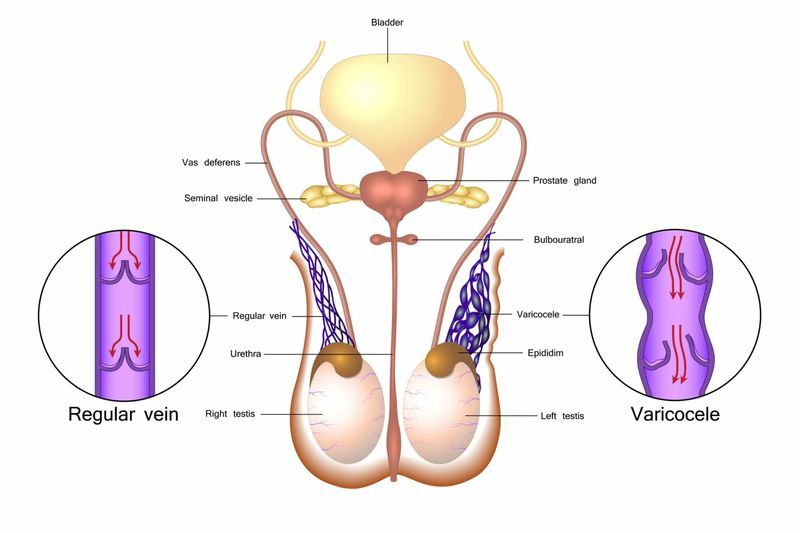
[Varicoceles](https://nabtahealth.com/glossary/varicoceles/) occur when the veins within the scrotum become enlarged. They usually develop around the time of [puberty](https://nabtahealth.com/glossary/puberty/) and are fairly common, affecting 10 to 15% of males. Usually they are [asymptomatic](https://nabtahealth.com/glossary/asymptomatic/) and will not require any treatment. However, they can grow over time causing pain, testicle shrinkage and/or [infertility](https://nabtahealth.com/glossary/infertility/). Up to 40% of men who struggle to conceive will discover they have [varicoceles](https://nabtahealth.com/glossary/varicoceles/). They are even more common in men who have secondary [infertility](https://nabtahealth.com/glossary/infertility/), i.e. those who experience difficulty in conceiving, having already fathered a child (or children). The prevalence in these cases is thought to be as high as 80%. #### **Why do [varicoceles](https://nabtahealth.com/glossary/varicoceles/) form?** Whilst the underlying mechanism is unclear, it is thought that [varicoceles](https://nabtahealth.com/glossary/varicoceles/) form when the valves within the veins hinder the flow of blood, causing it to pool, and the veins to swell. They more frequently occur on the left hand side, where the veins are under greater pressure to pump the blood back to the heart. #### **How are [varicoceles](https://nabtahealth.com/glossary/varicoceles/) diagnosed and treated?** [Varicoceles](https://nabtahealth.com/glossary/varicoceles/) are diagnosed via physical examination or ultrasound. When palpable, they are said to resemble a ‘bag of worms’. Approximately 20% of men who have [varicoceles](https://nabtahealth.com/glossary/varicoceles/) will struggle to conceive and, upon further testing, most of these men will also have abnormal semen. Not all cases of [varicoceles](https://nabtahealth.com/glossary/varicoceles/) will require treatment and many men remain [asymptomatic](https://nabtahealth.com/glossary/asymptomatic/) throughout life. However, in some cases the condition has been found to be progressive over time and as such, doctors often treat those with a palpable mass or a testicular size discrepancy of more than 20%, with a view to reducing the risk of future fertility problems. The preferred treatment approach is to perform a microscopic inguinal or subinguinal varicocelectomy. During this procedure, the surgeon will access the area via the groin and ligate the collateral veins, redirecting blood flow, but sparing the localised arteries and lymphatics. It has a low recurrence rate and seems to correlate well with an improvement in semen quality. #### **Why is it important to check for [varicoceles](https://nabtahealth.com/glossary/varicoceles/)?** It is concerning that a significant proportion of couples undergo Assisted Reproductive Technologies/Techniques ([ART](https://nabtahealth.com/glossary/art/)), which is financially, emotionally and physically draining, before checking for the presence of [varicoceles](https://nabtahealth.com/glossary/varicoceles/). In fact, in one review 70% of women who underwent [ART](https://nabtahealth.com/glossary/art/) had no abnormality in their reproductive system and the only clinical sign of [infertility](https://nabtahealth.com/glossary/infertility/) between the couple was [varicoceles](https://nabtahealth.com/glossary/varicoceles/) in the male partner. [ART](https://nabtahealth.com/glossary/art/) was never going to be successful in these cases. [Varicoceles](https://nabtahealth.com/glossary/varicoceles/) are common, but the good news is that their treatment is relatively straightforward and has a high success rate. Nabta is reshaping women’s healthcare. We support women with their personal health journeys, from everyday wellbeing to the uniquely female experiences of fertility, pregnancy, and [menopause](https://nabtahealth.com/glossary/menopause/). Get in [touch](/cdn-cgi/l/email-protection#126b737e7e73527c737066737a77737e667a3c717d7f) if you have any questions about this article or any aspect of women’s health. We’re here for you. **Sources:** * Balasubramanian, A, et al. “An Infertile Couple’s Long and Expensive Path to Varicocele Repair.” _Urology_, vol. 124, Feb. 2019, pp. 131–135., doi:10.1016/j.urology.2018.10.021. * Choi, W S, and S W Kim. “Current Issues in Varicocele Management: a Review.” _The World Journal of Men’s Health_, vol. 31, no. 1, Apr. 2013, pp. 12–20., doi:10.5534/wjmh.2013.31.1.12. * “What Are [Varicoceles](https://nabtahealth.com/glossary/varicoceles/)?” _Urology Care Foundation_, www.urologyhealth.org/urologic-conditions/[varicoceles](https://nabtahealth.com/glossary/varicoceles/).





























