
Towards the end of [pregnancies](https://nabtahealth.com/article/ectopic-pregnancies-why-do-they-happen/), many women try methods of natural induction. The evidence supporting various traditional methods is variable, and benefits, side effects, and notable potential health risks are present. Understanding what science says can help individuals make informed choices in consultation with a provider. Induction of Natural Labour induction Myths, Realities and Precautions ---------------------------------------------------------------------- The following section will review nine standard natural induction methods, discussing the proposed mechanism, evidence, and safety considerations. Avoid potential hazards by avoiding risky labor triggers and get advice from your [obstetrician](https://nabtahealth.com/glossary/obstetrician/) before choosing any method mentioned below. Castor Oil ---------- Castor oil has been used throughout the centuries to induce labor, and studies suggest that it does so on some 58% of occasions. This oil stimulates prostaglandin release, which in turn may have the result of inducing cervical changes. Adverse effects, such as nausea and [diarrhea](https://www.mayoclinic.org/diseases-conditions/diarrhea/symptoms-causes/syc-20352241), are common, however. Castor oil should be used near the [due date](https://nabtahealth.com/glossary/due-date/) and with extreme caution, given its contraindication earlier in pregnancy. Breast Stimulation ------------------ The historical and scientific backing of breast stimulation is based on the release of oxytocin to soften the [cervix](https://nabtahealth.com/glossary/cervix/). A study has shown that, with this method, cervical ripening may be achieved in about 37% of cases. However, excessive stimulation may cause uterine hyperstimulation, and guidance from professionals may be essential. Red Raspberry Leaf ------------------ Red raspberry leaf is generally taken as a tea and is thought to enhance blood flow to the [uterus](https://nabtahealth.com/glossary/uterus/) and stimulate [contractions](https://nabtahealth.com/glossary/contraction/). Traditional use, however, is tempered by a relative lack of scientific research regarding its effectiveness. Animal studies have suggested possible adverse side effects, and no human data are available that supports a correlation with successful induction of labor. Sex --- Sex is most commonly advised as a natural induction method based on the principle that sex introduces [prostaglandins](https://nabtahealth.com/glossary/prostaglandins/) and oxytocin, and orgasm induces uterine [contractions](https://nabtahealth.com/glossary/contraction/). The few studies in the literature report no significant effect on labor timing. Generally safe for women when pregnancy is otherwise low-risk but may not speed labor. Acupuncture ----------- Acupuncture is a traditional Chinese practice that has been done to stimulate labor through the induction of hormonal responses. However, some studies show its effectiveness in improving cervical ripening but not necessarily inducing active labor. An experienced practitioner would appropriately consult its safe application during pregnancy. Blue and Black Cohosh --------------------- Native American groups traditionally utilize blue and black cohosh plants for gynecological use. These plants are highly discouraged nowadays from inducing labor because of the risk of toxicity they may bring. Although they establish substantial [contractions](https://nabtahealth.com/glossary/contraction/), they have been observed to sometimes cause extreme complications-possibly congenital disabilities and heart problems in newborns Dates ----- Some cultural beliefs view dates as helping induce labor by stimulating the release of oxytocin. They do not help stimulate uterine [contractions](https://nabtahealth.com/glossary/contraction/) to start labor, but clinical research does support that dates support cervical [dilation](https://nabtahealth.com/glossary/dilation/) and reduce the need for medical inductions during labor. They also support less hemorrhaging post-delivery when consumed later in pregnancy. Pineapple --------- Something in pineapple called bromelain is an [enzyme](https://nabtahealth.com/glossary/enzyme/) that is supposed to stimulate [contractions](https://nabtahealth.com/glossary/contraction/) of the [uterus](https://nabtahealth.com/glossary/uterus/). Animal tissue studies have determined it would only work if applied directly to the tissue, so it’s doubtful this is a natural method for inducing labor. Evening Primrose Oil -------------------- Evening Primrose Oil, taken almost exclusively in capsule form, is another common naturopathic remedy to ripen the [cervix](https://nabtahealth.com/glossary/cervix/). Still, studies are very few and indicate a greater risk of labor complications, such as intervention during delivery, and it is not recommended very often. Safety and Consultation ----------------------- Many of these methods are extremely popular; however, most are unsupported by scientific data. Any method should be discussed with a healthcare provider because all may be contraindicated depending on gestational age, maternal health, and pregnancy risk levels. Try going for a walk, have a warm bath and relax while you’re waiting for your baby. “Optimal fetal positioning,” can help baby to come into a better position to support labor. You can try sitting upright and leaning forward by sitting on a chair backward. Conclusion ---------- Natural methods of inducing labor vary widely in efficacy and safety. Practices like breast stimulation and dates confer some benefits, while others, such as those involving castor oil and blue cohosh, carry risks. Based on the available evidence, decisions about labor induction through healthcare providers are usually the safest. You can track your menstrual cycle and get [personalised support by using the Nabta app](https://nabtahealth.com/nabta-app/). Get in touch if you have any questions about this article or any aspect of women’s health. We’re here for you. Sources : 1.S. M. Okun, R. A. Lydon-Rochelle, and L. L. Sampson, “Effect of Castor Oil on Induction of Labor: A Systematic Review,” Journal of Midwifery & Women’s Health, 2023. 2.T. K. Ford, H. H. Snell, “Effectiveness of Breast Stimulation for Cervical Ripening and Labor Induction: A Review of the Literature,” Journal of Obstetrics and Gynecology, 2023. 3.R. E. Smith, D. M. Wilson, “Red Raspberry Leaf and Its Role in Pregnancy and Labor: A Critical Review,” Alternative Medicine Journal, 2024. 4.A. L. Jameson, “Sexual Activity and Its Effect on Labor Induction: A Review,” International Journal of Obstetrics, 2023. 5.B. C. Zhang, Z. W. Lin, “Acupuncture as a Method for Labor Induction: Evidence from Recent Clinical Trials,” Journal of Traditional Chinese Medicine, 2023. 6.D. K. Patel, J. M. Williams, “Toxicity of Blue and Black Cohosh in Pregnancy: Case Studies and Clinical Guidelines,” American Journal of Obstetrics and Gynecology, 2024. 7.M. J. Abdullah, F. E. Azzam, “The Role of Dates in Pregnancy: A Review of Effects on Labor and Birth Outcomes,” Nutrition in Pregnancy, 2024. 8.S. L. Chung, L. M. Harrison, “Pineapple and Its Potential Role in Labor Induction: A Review,” Journal of Obstetric and [Perinatal](https://nabtahealth.com/glossary/perinatal/) Research, 2023. 9.L. M. Weston, A. R. Franklin, “Evening Primrose Oil for Labor Induction: A Comprehensive Review,” Journal of Alternative Therapies in Pregnancy, 2024. Patient Information Induction of labour Women’s Services. (n.d.). Retrieved November 9, 2024, from https://www.enherts-tr.nhs.uk/wp-content/uploads/2019/10/Induction-of-Labour-v5-09.2020-web.pdf

Is Performing a C-Section Better Than Inducing Labour, when it comes to giving birth, usually the preferred option is to let labour proceed naturally. However, there are times when it is not in the mother or baby’s interest for this to happen. When the health of either is at risk, or if gestation has exceeded [41 weeks duration,](https://nabtahealth.com/articles/doctor-tips-weeks-27-40/) then it is highly probable that an alternative strategy will need to be implemented. There are two options available, [inducing labour](../) or performing a [C-section](../). With an induction, the [uterus](https://nabtahealth.com/glossary/uterus/) is artificially stimulated to contract, and it is then hoped that labour will proceed as per a natural delivery. In contrast, a C-section is a surgical procedure, whereby a cut is made in the abdomen and the baby is removed that way, rather than via the [vagina](https://nabtahealth.com/glossary/vagina/). Sometimes the only safe option is to perform a C-section, for example if the baby is breach, or when an emergency situation arises. However, there are other times when you may be presented with a choice and if this happens, what is the correct answer? Unfortunately there is no definitive right answer. An induction can be at least as safe as spontaneous labour and, if performed in the week prior to the [due date](https://nabtahealth.com/glossary/due-date/), it is thought to reduce [the risk of](https://nabtahealth.com/articles/what-is-preeclampsia/) [preeclampsia](https://nabtahealth.com/glossary/preeclampsia/) in the mother and respiratory distress in the child, possibly as a result of the [placenta](https://nabtahealth.com/glossary/placenta/) remaining fully functional. Unlike C-sections, inductions are not surgical procedures and thus, if all goes to plan, the recovery period is shorter. It is however, a big ‘IF’. [Induced labours](https://nabtahealth.com/articles/induction-of-labour/) are typically more painful, meaning more women will request stronger pain relief including epidurals, and there is a greater likelihood of assisted delivery, such as the use of forceps or ventouse. There is also an increased [risk of hyperstimulation](https://nabtahealth.com/articles/what-is-ovarian-drilling/) of the [uterus](https://nabtahealth.com/glossary/uterus/)., Uterine hyperstimulation causes more frequent, longer [contractions](https://nabtahealth.com/glossary/contraction/), which can [lead](https://nabtahealth.com/glossary/lead/) to complications such as foetal heart rate abnormalities and, in rare cases, uterine rupture. In a significant number of women, induction does not work and a C-section becomes necessary. The advent of the C-section was undoubtedly a medical revolution, instantly saving the lives of millions of women and children. However, C-sections bring with them all the risks of regular surgery, including blood clots, wound infection and bleeding. The recovery period is typically longer after a C-section than after a natural birth, driving restrictions are enforced and a scar remains, although this will fade over time. Whilst current guidelines stipulate that an induction should only be performed when [the risks of continuing the pregnancy](https://nabtahealth.com/articles/complications-during-pregnancy-polyhydramnios/) outweighs the benefits, with more women than ever requesting elective C-sections, the World Health Organisation has highlighted an urgent need for medical assessment efforts to address the risks of induced labour compared to elective C-section. Until such work is undertaken, it becomes a matter of individual circumstance, personal choice and ultimately weighing up what is best for you and your baby. **Sources:** * Grobman, W A, et al. “Labor Induction versus Expectant Management in Low-Risk Nulliparous Women.” _The New England Journal of Medicine_, vol. 379, no. 6, 9 Aug. 2018, pp. 513–523., doi:10.1056/NEJMoa1800566. * WHO Recommendations for Induction of Labour. World Health Organisation, [http://apps.who.int/iris/bitstream/handle/10665/44531/9789241501156\_eng.pdf?sequence=1](http://apps.who.int/iris/bitstream/handle/10665/44531/9789241501156_eng.pdf?sequence=1). Accessed on 23/01/2019. * _Inducing Labour. Clinical Guideline \[CG70\]_. NICE (National Institute for Care and Health Excellence), July 2008, www.nice.org.uk/guidance/cg70/chapter/Introduction. Accessed on 23/01/2019

* Jasmine Collin from [Love Parenting UAE](https://www.loveparentinguae.com/), Nabta Health’s hypnotherapy partner, takes us through her guide to all things Hypnobirthing. * Learn how Hypnobirthing supports natural birth, reducing pain and creating an optimal environment during labour. * Nabta’s aim to empower women to reach their health goals as naturally as possible is very much in line with Jasmine’s approach and the benefits of hypnotherapy in labour. * Book Jasmine’s popular online Hypnobirthing course [here.](https://nabtahealth.com/product/the-love-birthing-hypnobirthing-course/) You may have heard of hypnobirthing due to its increasing popularity with expecting parents and [celebrities such as Jessica Alba and Angelina Jolie.](https://www.madeformums.com/pregnancy/celebrity-mums-who-used-hypnotherapy-in-labour/) It’s even been suggested that royal family members, Kate Middleton and Meghan Markle used it to prepare for their births – but what exactly is it and why are so many women turning to Hypnobirthing? **What is Hypnobirthing?** Hypnobirthing is a childbirth preparation method taken as a set of weekly classes either in groups or privately, any time between 20-35 weeks of pregnancy. There are lots of styles of Hypnobirthing available today but they all originate from the Mongan Method, which is over 30 years old. There are also online Hypnobirthing classes available too There are a lot of [misconceptions as to what Hypnobirthing](https://www.loveparentinguae.com/single-post/2019/10/07/why-there-is-no-such-thing-as-a-hypnobirth) is and the type of person who chooses it. Many think it’s just for hippy types wanting a home or [water birth](https://nabtahealth.com/glossary/water-birth/) or those seemingly crazy women who want to do it without pain relief, but the truth is, all women can use it to have a calmer more positive birth experience, no matter what birth they choose or what path it takes. **What is the aim of Hypnobirthing?** One of the aims of Hypnobirthing is to support and increase the likelihood of physiological birth with the least amount of chemicals and interventions wherever possible. However if drugs or medical interventions are truly needed it enables the couple to remain calm and make informed evidence based decisions for themselves and their baby. #### **What are the benefits of natural physiological birth?** Studies have shown us that women and babies who have natural physiological births benefit from better health outcomes, adjustment to life outside the womb, emotional satisfaction with the birth experience and being able to cope well with the transition to motherhood. Read more about [physiological birth](http://www.birthtools.org/What-Is-Physiologic-Birth) and its benefits for families and society as a whole. Hypnobirthing promotes births that mirror nature as closely as possible so that babies and families can get off to the best start possible. #### **What if natural birth is not possible?** Unfortunately, natural physiological birth is not always possible in our current birth culture. There are a large number of influencing factors that we can’t control and birth can be quite unpredictable. So it’s important to acknowledge the wide range of birthing styles, combinations of drugs, interventions and different experiences that can happen, so we can fully prepare couples for all eventualities. The great news is that the knowledge and techniques learnt in Hypnobirthing classes are applicable in all situations and in all types of birth. In fact the tools can be even more useful in assisted births like C- sections, epidurals and inductions etc. because they keep the mother and baby calm during potentially more stressful events. #### **Real Hypnobirthing stories** Here are a few birth stories from parents who had all types of birthing experiences and how Hypnobirthing helped them through. [The induction for](https://babyandchild.ae/uae-birth-guide/article/1523/labour-was-more-powerful-and-beautiful-than-i-could-have-imagined) [gestational diabetes](https://nabtahealth.com/glossary/gestational-diabetes/) one [The induction and low](https://www.jasminecollin.com/single-post/2019/05/06/Taylors-Birth---A-calm-positive-tale-of-thrombocytopenia-induction-low-fluid-and-more) [amniotic fluid](https://nabtahealth.com/glossary/amniotic-fluid/) one [The planned gentle C-section one](https://www.jasminecollin.com/single-post/2017/04/16/Hanis-Birth---A-Family-Centred-Cesarean) [The one with no progress](https://www.jasminecollin.com/single-post/2017/05/04/Charleys-Birth) [The big baby one](https://babyandchild.ae/uae-birth-guide/birth-stories/article/1372/how-hypnobirthing-helped-me-give-birth-to-my-5kg-baby-drug-free) [The unplanned C-section one](https://www.jasminecollin.com/single-post/2015/05/10/10-Healthy-Foods-That-Calm-DeStress) [The VBA2C (Vaginal Birth after 2 C sections) one](https://www.jasminecollin.com/single-post/2017/04/23/Marsels-Birth---A-VBA2C-Story) [The planned vaginal](https://www.jasminecollin.com/single-post/2017/08/13/Phoenix-Willows-Breech-Birth) [breech](https://nabtahealth.com/glossary/breech/) one [The unplanned vaginal](https://www.jasminecollin.com/single-post/2017/01/26/Georges-Breech-Birth) [breech](https://nabtahealth.com/glossary/breech/) one As you can read in the birth stories, Hypnobirthing can benefit mothers and babies in all situations – but it’s not just them that benefit. Let’s not forget the partners. These days’ partners are not just welcome in the delivery room; they are expected to support the mother during labour and birth. However, without adequate training this can throw them into an environment and situation that they are not adequately prepared for. In Hypnobirthing classes partners gain invaluable knowledge and skills that they can apply in the birthing room to ensure a positive birth experience for the mother, baby and themselves. And the benefits don’t just stop in the birthing room. Lots of couples continue to use the tools for relaxing the mind and body long after the birth is over. Read- [7 surprising reasons to do Hypnobirthing that have nothing to do with birth](http://www.loveparentinguae.com/single-post/2017/08/02/7-Surprising-Reasons-To-Do-Hypnobirthing-Classes-That-Have-Nothing-To-Do-With-Birth) #### **So how does Hypnobirthing work exactly?** **During pregnancy** It empowers couples with the knowledge and belief that women’s bodies are designed to grow and birth their babies and that childbirth is a natural physiological process. It promotes healthy nutrition and physical exercise in pregnancy as being key factors in having a safe and easier birth as well sharing top tips on how to get the baby into the optimal position for birthing. Like any big physical event such as running a marathon or climbing a mountain, it’s not just physical preparation that makes the difference. Yes, physical fitness plays a big part, but a positive mindset and being emotional fit is just as important, and this is where Hypnobirthing comes in. Hypnobirthing de-hypnotises couples from all the negative information and fear that they’ve been conditioned with all their lives and updates their mindset through guided visualisations, affirmations and fear release work, all while they are very deeply relaxed or ‘in hypnosis’. Being in a natural state of hypnosis, promotes deep relaxation and being open to suggestion, so during pregnancy we can give the mind set an upgrade by accessing the sub conscious mind and reprograming it with more positive beliefs, thoughts and feelings about birth. When pregnant woman are calm and feel fully supported, their babies, who are literally swimming in their emotions, also feel the benefits. During classes there is also a focus on pre birth family bonding and this helps couples to adjust to their new roles and embrace early parenthood more easily. #### **Hypnobirthing during labour & birth** When a woman goes into labour with less fear and more understanding of how her body works and what it’s doing at each stage she can accept it more easily and experience it in a more positive way. When she relaxes and welcomes the sensations, rather than fighting them, they can then become easier to manage. Practically speaking Hypnobirthing teaches couples how to maximize the normal physiological birth process by creating the optimal environment for birth. Humans are biologically programmed in the same way that all mammals are and our birth environment needs are very similar. All mammals birth more easily in safe, warm, dark, private, quiet and undisturbed settings where there is no rush and no feeling of being watched or observed. In this ideal setting the perfect and natural combination of birthing hormones can be released and labour can progress. If however there is any sense of a potential threat or disturbance, our fight or flight response can release hormones that will slow or even stop labour. Even a bright light or a cold room is enough to slow down labour. It’s not always possible to control the external environment though, for example when driving to the hospital or in a typical hospital room, where it’s normally bright, busy and rushed, with lots of observation, disturbances and possible fear triggers. Hypnobirthing skills are crucial in these less than optimal settings because they enable the mother to create a calm and resourceful internal mental state. Using her practiced breathing, visualisations, affirmations and hypnosis she can bring her body and mind into a deep state of relaxation as if she were in the ideal environment. The body cannot tell the difference between real and imagined, so she can use this mind-body hack to convince her body that it’s a safe space and a good time to be birthing her baby. The body then continues releasing the perfect cocktail of hormones for a quicker, easier and more natural birth. #### But what about the pain? A birthing mother automatically reduces pain by being calmer and less frightened of the birth, and in calm, safe settings the birthing body naturally produces [endorphins](https://nabtahealth.com/glossary/endorphins/), our own natural pain relief, to help us cope with the intense physical sensations. In addition, Hypnobirthing mums can use hypnosis to disrupt and change the way that their brain processes pain signals. They also learn mental coping strategies and physical comfort tools to deal with any discomfort that they feel. All these factors make it less likely that they will need pain relieving drugs or unnecessary interventions and they tend to have more straightforward and quicker labours. Of course if a woman is struggling then there is a selection of pain relieving drugs that the hospital can offer. The aim of Hypnobirthing however is to ensure the couple have a complete toolbox of skills and techniques that they can utilize before getting to that point, so that it can be delayed or avoided all together. But, no matter how a baby is born or whatever interventions or drugs are used, the most important elements for every birthing mother are that: * She feels calm, safe, and supported throughout. * She feels that she did her best and gave it all she had. * She feels treated with dignity and respect. * And she was able to make her own informed choices about her baby, body and birth, every step of the way. These are the key ingredients to a positive birth experience and what Hypnobirthing is all about. Surely every mother and her family deserves this birth experience…not just the hippies. \_\_\_\_\_ Jasmine Collin is a mother of two, a qualified Hypnotherapist, NLP Practitioner, Childbirth Educator and Doula who specialises in Hypnobirthing and Parenting Originally from the UK she is the longest running teacher in the UAE and has been teaching her award winning ‘Love Birthing’ classes since 2009. She is the co founder of Love Parenting UAE, winner of the 2018 Time Out Kids Award for ‘Special recognition for pre and post natal care’ and is dedicated to helping couples have calmer, more positive births so that they can ‘Love Birthing’ no matter what kind of birth they choose or what path birth takes. For more information contact: [\[email protected\]](/cdn-cgi/l/email-protection) You can book Jasmine’s popular online Hypnobirthing services on the [Nabta Women’s Health Shop.](https://nabtahealth.com/product/the-love-birthing-hypnobirthing-course/) \_\_\_ Nabta is reshaping women’s healthcare. We support women with their personal health journeys, from everyday wellbeing to the uniquely female experiences of fertility, pregnancy, and [](https://nabtahealth.com/glossary)[menopause](https://nabtahealth.com/glossary/menopause/). You can track your menstrual cycle and get [personalised support by using the Nabta app.](https://nabtahealth.com/our-platform/nabta-app/) Get in [touch](/cdn-cgi/l/email-protection#acd5cdc0c0cdecc2cdced8cdc4c9cdc0d8c482cfc3c1) if you have any questions about this article or any aspect of women’s health. We’re here for you.

Childbirth is a remarkable journey, and expectant parents have several options when it comes to deciding how and where they want to bring their baby into the world. One such option gaining popularity is water births. This method involves giving birth in a specially designed tub or pool filled with warm water. In this article, we will explore what [water birth](https://nabtahealth.com/glossary/water-birth/) is, its potential benefits, and some important factors to consider. #### What is [Water Birth](https://nabtahealth.com/glossary/water-birth/)? [Water Birth](https://nabtahealth.com/glossary/water-birth/) refers to the process of giving birth in a birthing pool or tub filled with warm water. It can take place at home, in a birthing center, or even in a [hospital setting](https://nabtahealth.com/articles/are-home-births-safe/). During a [water birth](https://nabtahealth.com/glossary/water-birth/), the expectant mother immerses herself in the water, allowing her body to relax and her muscles to ease tension. #### Benefits of [Water Birth](https://nabtahealth.com/glossary/water-birth/): **Natural pain relief:** The warm water helps to relax the body and release [endorphins](https://nabtahealth.com/glossary/endorphins/), which are natural pain-relieving hormones. Many women find that being in water during labor helps them manage their pain and discomfort. **Promotes relaxation:** Immersion in water promotes a sense of deep relaxation, reducing anxiety and stress during labor. Relaxation can help facilitate a smoother birth process and may even [lead](https://nabtahealth.com/glossary/lead/) to a shorter labor. **Improved blood circulation:** The water’s buoyancy helps reduce pressure on the mother’s body, allowing for better blood circulation and optimal oxygen supply to both the mother and baby. **Increased mobility:** The weightlessness and freedom of movement in water can make it easier for the mother to change positions, promoting optimal fetal positioning and facilitating a smoother descent of the baby through the birth canal. **Gentle transition for the baby:** Babies spend nine months in the [amniotic fluid](https://nabtahealth.com/glossary/amniotic-fluid/) within the womb, and being born into warm water can provide a gentle transition into the outside world, mimicking the familiar environment of the womb. #### Important Considerations: **Consult with healthcare professionals:** It is crucial to consult with your healthcare provider, such as an [obstetrician](https://nabtahealth.com/glossary/obstetrician/) or midwife, to determine if [water birth](https://nabtahealth.com/glossary/water-birth/) is a suitable option for you. They will assess your medical history and discuss any potential risks or contraindications. **[Water birth](https://nabtahealth.com/glossary/water-birth/) settings:** It can take place at home, birth centers, or certain hospitals. It is essential to choose a facility that supports and has experience with water deliveries, ensuring that the necessary equipment and professionals are available. **Preparation and education:** Attending childbirth education classes that specifically cover [water birth](https://nabtahealth.com/glossary/water-birth/) can help you understand the process, learn breathing and relaxation techniques, and familiarize yourself with the [benefits and potential challenges](https://nabtahealth.com/articles/are-home-births-safe/) associated with water delivery. **Partner and support person involvement:** Discuss the role of your partner or support person during the birth. They can provide emotional support, assist with positioning, and ensure your comfort throughout the process. **Safety measures:** The water temperature should be maintained between 95-100 degrees Fahrenheit (35-37 degrees Celsius) and regularly monitored. The tub or pool should be clean and sanitized to prevent infections. **Alternatives to [water birth](https://nabtahealth.com/glossary/water-birth/):** It is important to note that even if you plan for a water delivery, circumstances may arise during labor that necessitate [alternative methods](https://deltastrengthdoula.com/) of delivery. Flexibility and open communication with your healthcare team are vital in such situations. [Water birth](https://nabtahealth.com/glossary/water-birth/) offers an alternative birthing option for expectant mothers seeking a natural and calming experience. The warm water provides pain relief, promotes relaxation, and allows for greater mobility during labor. However, it is essential to consult with healthcare professionals, evaluate the suitability for water delivery based on individual circumstances. Ensuring a safe and supportive environment for this birthing method. With the proper preparations and precautions, water delivery can be a beautiful and empowering choice for women welcoming their little ones into the world.

Postnatal exercise can help you recover after childbirth, make you stronger and improve your mood. Even if you’re tired and not feeling motivated, there’s plenty you can do to get your body moving. But no 2 pregnancies are the same. How soon you’re ready to start exercising depends on your individual circumstances. You should always check with a health professional first. When you feel ready to exercise, it’s very important to not overdo it. [Your body](https://www.pregnancybirthbaby.org.au/what-happens-to-your-body-in-childbirth) has been through some big changes. You will need time to recover, even if you’re feeling great after having your baby. **Why should I do pelvic floor exercises after birth?** Pelvic floor exercises are important at all stages of life to prevent bladder and bowel problems, such as incontinence and prolapse, and improve sexual function. Your [pelvic floor](https://www.pregnancybirthbaby.org.au/anatomy-of-pregnancy-and-birth-perineum-pelvic-floor) is a group of muscles which support your bladder, [](https://www.pregnancybirthbaby.org.au/anatomy-of-pregnancy-and-birth-uterus)[uterus](https://nabtahealth.com/glossary/uterus/) and bowel. These muscles form a ‘sling’ which attaches to your pubic bone at the front and your tailbone at the back. Your urethra, [vagina](https://nabtahealth.com/glossary/vagina/) and anus, all pass through the pelvic floor. In pregnancy, hormonal changes cause your muscles to soften and stretch more easily. These changes, along with the weight of your growing baby, put extra strain on the pelvic floor. Labour and birth can also weaken your pelvic muscles. This can increase the chance of suffering from [bladder or bowel problems](https://www.pregnancybirthbaby.org.au/bladder-and-bowel-problems-during-pregnancy) during pregnancy and after birth. Gentle exercise to restore your pelvic health is the best way to begin and you can gradually increase the intensity [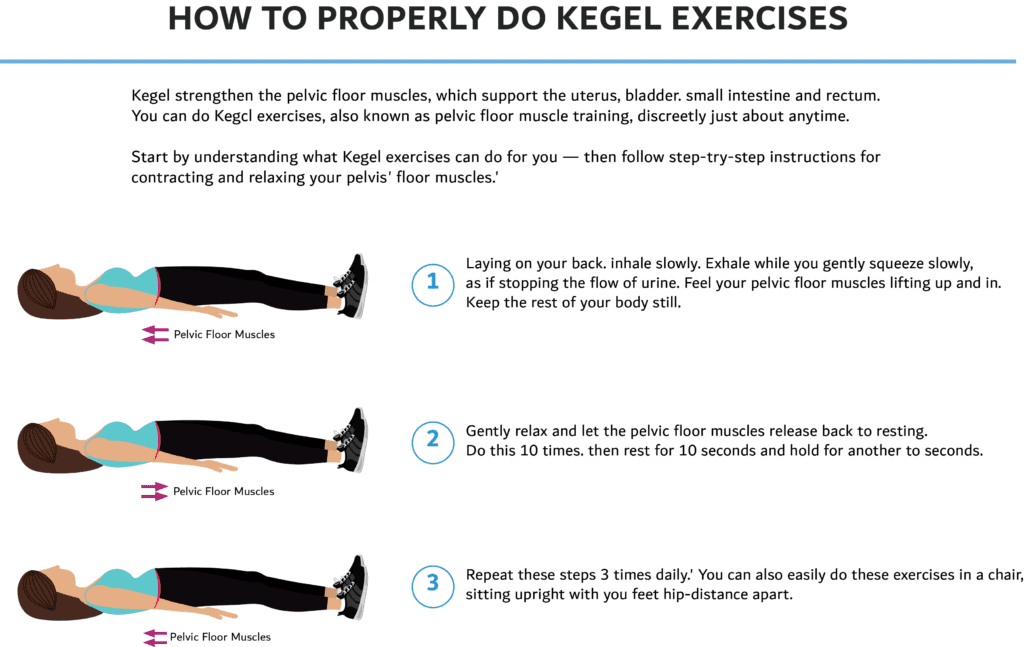](https://nabtahealth.com/wp-content/uploads/2023/03/Kegel-Exersices-PNG-1024x647-1.png) **What type of exercises can I do?** Do More: 1. Gentle exercise such as walking can be done as soon as you feel comfortable after giving birth 2. Start with easy exercises and gentle stretches and slowly build up to harder ones 3. Other safe exercises include swimming (once bleeding has stopped), yoga, pilates, low impact aerobics and cycling Avoid: 1. Any high intensity exercises or sports that require rapid direction changes 2. Stretching and twisting too vigorously to prevent injury 3. Heavy weights, sit ups, crunches and planks for 3 months #### Goals of a well designed Postpartum Exercise program 1. Rest and recover 2. Maintain good posture and alignment 3. Rehabilitate the pelvic floor muscles 4. Increase strength especially in the core muscles At Nabta Health Clinic, we have specialized exercise packages which include pelvic floor rehabilitation and pilates exercise program for pregnancy and the postnatal period to help you in your well being and recovery. Nabta is reshaping women’s healthcare. We support women with their personal health journeys, from everyday wellbeing to the uniquely female experiences of fertility, pregnancy, and [](https://nabtahealth.com/glossary)[menopause](https://nabtahealth.com/glossary/menopause/). You can [email us](/cdn-cgi/l/email-protection#235a424f4f42634d424157424b46424f574b0d404c4e) or call us at **+971 4 3946122** for more information

Pregnancy linked to developing cervical cancer, The Lancet is one of the most widely read and well regarded medical journals and, as a result, work that gets published within it is generally considered to be high quality and scientifically robust. In 2002, the Lancet published the results of a study looking at the effects of parity (the number of times a woman has been pregnant and carried the baby to a viable [gestational age](https://nabtahealth.com/articles/gestational-diabetes-8-things-you-should-know/)) on cervical cancer rates. This followed work from the late 1980s and early 1990s that suggested that women who had been pregnant multiple times were more susceptible to _cervical cancer_. The findings published in the Lancet revealed that for [HPV](https://nabtahealth.com/glossary/hpv/)\-positive women there was a direct association between number of full-term pregnancies and risk of developing cervical cancer. This supported earlier work that stated that the risk of cervical cancer was more than 2-fold higher in women who had four or more children, compared to those who had none or one. **There are a few key points to note:** * The women at greatest risk are those who experience persistent [HPV](https://nabtahealth.com/glossary/hpv/) infection. High parity seems to act as a cofactor, interacting with [HPV](https://nabtahealth.com/glossary/hpv/) to induce cervical carcinoma. The relative risk is much lower in women who are [HPV](https://nabtahealth.com/glossary/hpv/)\-negative. * There is no evidence that high parity increases the risk of [HPV](https://nabtahealth.com/glossary/hpv/) infection. * The association is only seen with pregnancies classed as full-term. It is, therefore, likely, that the events triggering [carcinoma](https://www.cancercenter.com/carcinoma) progression happen during the second or third trimester, or even during delivery. It has been suggested that women who deliver vaginally are at a slightly higher risk than those who have a [caesarean](https://nabtahealth.com/glossary/caesarean/) section, however, this data is limited and the theory requires further validation. * Other factors may confound, or exacerbate the effect; for example, it has been suggested that prolonged [oral contraceptive](../the-oral-contraceptive-pill) use might have a multiplicative effect, increasing the risk further in women who are multiparous. Not all studies have identified a positive link; some do not find a significant association and others only find a link between high parity and certain types of cervical carcinoma. Some of the studies fail to consider whether a female has undergone frequent [pap screening](../when-should-i-get-a-pap-smear), or how many previous partners she has had. The biggest risk factor for the development of [HPV](https://nabtahealth.com/glossary/hpv/) is having multiple sexual partners. This data appears sound, even though the reported values are likely to be an under-estimation, due to an unwillingness of women to disclose this type of information. #### **Biological mechanism** There are plausible mechanisms for an involvement of pregnancy in the transition of normal cervical cells into cancerous lesions. [High risk](https://nabtahealth.com/articles/human-papillomavirus-hpv-and-cervical-cancer/) [HPV](https://nabtahealth.com/glossary/hpv/) infection is implicated in almost all cases of cervical cancer. However, not all women with [HPV](https://nabtahealth.com/glossary/hpv/) go on to develop cancer. It is thought that the high levels of [oestrogen](https://nabtahealth.com/glossary/oestrogen/) and [progesterone](https://nabtahealth.com/glossary/progesterone/) present throughout pregnancy, but particularly high in the last few weeks, cause cellular transformations on the surface of the [cervix](https://nabtahealth.com/glossary/cervix/) that last many years. This can cause prolonged exposure of the transformation zone in the [cervix](https://nabtahealth.com/glossary/cervix/) to [HPV](https://nabtahealth.com/glossary/hpv/) and increase the likelihood of persistent infection and progression to cancer. Another consideration is that the immunosuppression that is a natural part of pregnancy, can enhance the role of [](https://nabtahealth.com/articles/human-papillomavirus-hpv-and-cervical-cancer/)[HPV](https://nabtahealth.com/glossary/hpv/) in cervical carcinogenesis. One important theory proposed by the authors of the aforementioned Lancet study, is that smaller family sizes might explain, in part, why there has been a global decline in cervical cancer mortality and incidence. This decline is considered to be mainly due to an increased awareness of pap screening as well as the advent of the hugely effective [](../can-cervical-cancer-be-prevented)[HPV](https://nabtahealth.com/glossary/hpv/) vaccine; however, in countries where screening rates are low and the vaccine has not yet been introduced, a reduction in parity rates may provide an explanation. Nabta is reshaping women’s healthcare. We support women with their personal health journeys, from everyday wellbeing to the uniquely female experiences of fertility, pregnancy, and [menopause](https://nabtahealth.com/glossary/menopause/). Get in [touch](/cdn-cgi/l/email-protection#fd849c91919cbd939c9f899c95989c918995d39e9290) if you have any questions about this article or any aspect of women’s health. We’re here for you. **Sources:** * Brinton, Louise A., et al. “Parity As A Risk Factor For Cervical Cancer.” _American Journal of Epidemiology_, vol. 130, no. 3, Sept. 1989, pp. 486–496., doi:10.1093/oxfordjournals.aje.a115362. * Jensen, K E, et al. “Parity as a Cofactor for High-Grade Cervical Disease among Women with Persistent Human Papillomavirus Infection: a 13-Year Follow-Up.” _British Journal of Cancer_, vol. 108, no. 1, 15 Jan. 2013, pp. 234–239., doi:10.1038/bjc.2012.513. * Kasamatsu, Elena, et al. “Factors Associated with High-Risk Human Papillomavirus Infection and High-Grade Cervical Neoplasia: A Population-Based Study in Paraguay.” _Plos One_, vol. 14, no. 6, 27 June 2019, doi:10.1371/journal.pone.0218016. * Muñoz, Nubia, et al. “Role of Parity and Human Papillomavirus in Cervical Cancer: the IARC Multicentric Case-Control Study.” _The Lancet_, vol. 359, no. 9312, 30 Mar. 2002, pp. 1093–1101., doi:10.1016/s0140-6736(02)08151-5. * Roura, Esther, et al. “The Influence of Hormonal Factors on the Risk of Developing Cervical Cancer and Pre-Cancer: Results from the EPIC Cohort.” _Plos One_, vol. 11, no. 1, 25 Jan. 2016, doi:10.1371/journal.pone.0147029. * Russo, Evandro, et al. “Vaginal Delivery and Low Immunity Are Strongly Associated With High-Grade Cervical Intraepithelial Neoplasia in a High-Risk Population.” _Journal of Lower Genital Tract Disease_, vol. 15, no. 3, July 2011, pp. 195–199., doi:10.1097/lgt.0b013e31820918ea. * Trottier, Helen, et al. “Risk of Human Papillomavirus ([HPV](https://nabtahealth.com/glossary/hpv/)) Infection and Cervical Neoplasia after Pregnancy.” _BMC Pregnancy and Childbirth_, vol. 15, no. 1, 7 Oct. 2015, doi:10.1186/s12884-015-0675-0.

* [Stillbirth](https://nabtahealth.com/glossary/stillbirth/) is the loss of a baby in the womb after 24 weeks of pregnancy. * Every year there are an estimated 2.6 million stillbirths worldwide. * One third of stillbirths are unexplained. Around a quarter are caused by birth defects. Other risk factors include higher age, drug use and multiples. * Early warning signs of [stillbirth](https://nabtahealth.com/glossary/stillbirth/) include change the baby’s movements, bleeding, itching, fever and headaches. One [stillbirth](https://nabtahealth.com/glossary/stillbirth/) tragically occurs every 16 seconds according to the [World Health Organisation (WHO)](https://www.who.int/health-topics/stillbirth#tab=tab_3). The [National Institutes of Health (NIH)](https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5139804/) acknowledges that there is no universally accepted definition for when a fetal death is called a [stillbirth](https://nabtahealth.com/glossary/stillbirth/). Rather than a [miscarriage](https://nabtahealth.com/glossary/miscarriage/) and the interpretation of gestational age differs by country. What causes [stillbirth](https://nabtahealth.com/glossary/stillbirth/)? ----------------------------------------------------------------------- [Around one third of stillbirths are unexplained](https://my.clevelandclinic.org/health/diseases/9685-stillbirth). According to the Centers for Disease Control and Prevention (CDC) [](https://www.cdc.gov/ncbddd/stillbirth/facts.html)[stillbirth](https://nabtahealth.com/glossary/stillbirth/) can happen to women of any age, background or ethnicity. The CDC goes on to say that the loss of a baby due to [stillbirth](https://nabtahealth.com/glossary/stillbirth/) occurs more commonly among: * Women with a higher maternal age; * Women who smoke or use recreational drugs during pregnancy; * Black women; * Women of a low [socioeconomic](https://nabtahealth.com/glossary/socioeconomic/) status; * Women who are pregnant with multiples (twins, triplets and quadruplets); and, * Women who have had a previous pregnancy loss. Blood-clotting disorders and chronic diseases (diabetes, heart disease, [lupus](https://nabtahealth.com/glossary/lupus/), obesity and thyroid disease) are also linked with increased risk of [stillbirth](https://nabtahealth.com/glossary/stillbirth/). As are complications with the [placenta](https://nabtahealth.com/glossary/placenta/) and [umbilical cord](https://nabtahealth.com/glossary/umbilical-cord/), maternal infections (group B streptococcus, [malaria](https://nabtahealth.com/glossary/malaria/), [HIV](https://nabtahealth.com/glossary/hiv/) and some STDs) and physical trauma. ##### Research says; [The Cleveland Clinic](https://my.clevelandclinic.org/health/diseases/9685-stillbirth) says birth defects are the cause of around 25% of stillbirths. While Tommy’s says that [failure of the](https://www.tommys.org/baby-loss-support/stillbirth-information-and-support/causes-stillbirth) [placenta](https://nabtahealth.com/glossary/placenta/) is the most common known reason for a baby to be stillborn. Half of all stillbirths linked to complications with the [placenta](https://nabtahealth.com/glossary/placenta/). The risk of the [placenta](https://nabtahealth.com/glossary/placenta/) calcifying increases when the baby reaches [full term](https://nabtahealth.com/glossary/full-term/). Over half of all placentas will experience some degree of calcification at [full term](https://nabtahealth.com/glossary/full-term/). Placental calcification preterm ranges wildly – from 3.8 to 23.7 percent – based on the risk factors listed above. What are the warning signs of [stillbirth](https://nabtahealth.com/glossary/stillbirth/)? ----------------------------------------------------------------------------------------- [Stillbirth](https://nabtahealth.com/glossary/stillbirth/) can occur without any obvious indicators but there are some signs to look for. If you experience any of the below symptoms during your pregnancy you should contact your medical team immediately. * **Change in baby’s movements**: Most women will start to feel the flutterings of their baby moving anywhere from 16 weeks onwards. By around 24 weeks the baby’s movements will be becoming more regular. [UK charity Tommy’s](https://www.tommys.org/baby-loss-support/stillbirth-information-and-support/stillbirth-symptoms-and-risks) recommends that you learn to recognise your baby’s pattern of movements in the womb. Some women notice that their baby seems more active in the evenings. This is when they sit down and put their feet up or in response to the music beat during an exercise class. Others find their baby’s kicks increase when they eat spicy foods or drink a large glass of cold juice. The important point here is that if you notice any change in your baby’s movements – if the kicks suddenly seem less frequent or not as strong as usual – you should contact your doctor immediately. As this may be a sign that your baby is not getting enough oxygen or nutrients. * **Vaginal spotting or bleeding and cramping:** This could be the sign of placental abruption, [a serious condition in which the](https://www.marchofdimes.org/complications/placental-abruption.aspx) [placenta](https://nabtahealth.com/glossary/placenta/) separates from the wall of the [uterus](https://nabtahealth.com/glossary/uterus/) before birth. * **Vaginal discharge or fluid leaking from the [vagina](https://nabtahealth.com/glossary/vagina/)**: Discharge could be linked with an intrauterine infection or infection in the womb. Leaking fluid could be your waters breaking early. * **Feeling something in your [vagina](https://nabtahealth.com/glossary/vagina/) during pregnancy:** This might be the sign of an [umbilical cord](https://nabtahealth.com/glossary/umbilical-cord/) prolapse which would mean your baby isn’t getting enough oxygen. * **Itching:** Severe itching on your palms and soles of your feet may be a sign of Intrahepatic Cholestasis of Pregnancy (IHP). It is a pregnancy-related liver condition that can [lead](https://nabtahealth.com/glossary/lead/) to [stillbirth](https://nabtahealth.com/glossary/stillbirth/). Also called obstetric cholestasis you should report any itching to your physician. * **Fever:** Some infections during pregnancy can be dangerous for an unborn baby. * **Headaches, blurred vision or swelling:** These can be [symptoms of](https://nabtahealth.com/articles/what-is-preeclampsia/) [preeclampsia](https://nabtahealth.com/glossary/preeclampsia/) which can [lead](https://nabtahealth.com/glossary/lead/) to loss of pregnancy in the womb. Your medical team will monitor your symptoms including carrying out an ultrasound to check your baby and using a [doppler ultrasound](https://nabtahealth.com/glossary/doppler-ultrasound/) to measure the fetal heart rate. It is important that you attend all your routine antenatal tests and scans and report any concerns or unusual symptoms you have. However slight you feel they may be, as soon as you notice them. Getting the support you need after [stillbirth](https://nabtahealth.com/glossary/stillbirth/) --------------------------------------------------------------------------------------------- Losing a baby at any stage is devastating and it is important that you, your partner and family get the physical and emotional support you need. Your [healthcare team](https://nabtahealth.com/team/) will be able to advise on the local support networks and dedicated charities there to support you. — Nabta is reshaping [women’s healthcare](https://nabtahealth.com/). We support women with their personal health journeys, from everyday wellbeing to the uniquely female experiences of fertility, pregnancy, and [](https://nabtahealth.com/glossary)[menopause](https://nabtahealth.com/glossary/menopause/). You can track your symptoms and get [personalised support by using the Nabta app.](https://nabtahealth.com/our-platform/nabta-app/) Get in [touch](/cdn-cgi/l/email-protection#740d15181815341a151600151c111518001c5a171b19) if you have any questions about this article or any aspect of women’s health. We’re here for you. **Sources** “[Stillbirth](https://nabtahealth.com/glossary/stillbirth/)” The Cleveland Clinic https://my.clevelandclinic.org/health/diseases/9685-[stillbirth](https://nabtahealth.com/glossary/stillbirth/) “[Stillbirth](https://nabtahealth.com/glossary/stillbirth/)” WHO, [https://www.who.int/health-topics/](https://www.who.int/health-topics/stillbirth#tab=tab_3)[stillbirth](https://nabtahealth.com/glossary/stillbirth/)#tab=tab\_3 Tavares da Silva, F, “[Stillbirth](https://nabtahealth.com/glossary/stillbirth/): Case definition and guidelines for data collection, analysis, and presentation of maternal immunization safety data” Dec 2016, Vaccine, [https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5139804/](https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5139804/) “What is [Stillbirth](https://nabtahealth.com/glossary/stillbirth/)” CDC https://www.cdc.gov/ncbddd/[stillbirth](https://nabtahealth.com/glossary/stillbirth/)/facts.html “Causes of [Stillbirth](https://nabtahealth.com/glossary/stillbirth/)” Tommy’s, https://www.tommys.org/baby-loss-support/[stillbirth](https://nabtahealth.com/glossary/stillbirth/)\-information-and-support/causes-[stillbirth](https://nabtahealth.com/glossary/stillbirth/)

Is it period while you’re pregnant, First of all, * It is normal for around a third of [pregnant](https://nabtahealth.com/articles/ectopic-pregnancies-why-do-they-happen/) women to experience spotting or light bleeding. This is not a period. * When you [become pregnant](https://nabtahealth.com/articles/how-do-pregnancy-tests-work/), you hormones will prevent [ovulation](https://nabtahealth.com/glossary/ovulation/) and therefore you will not have periods. Is it a myth that pregnant women don’t have periods? ---------------------------------------------------- In short, no! You cannot get period while you’re pregnant. Both your period and [pregnancy](https://nabtahealth.com/articles/getting-started-with-nabta-health-your-101-guide-to-pregnancy-week-by-week/) cause fluctuations in hormones. Because both events can bring on their own unique set of challenges, it’s easy to wonder if you can expect to get your [period](https://nabtahealth.com/articles/why-are-my-periods-irregular/)—or something like it—while you’re pregnant. About 25-30 percent of women will have light bleeding in [pregnancy](https://nabtahealth.com/articles/how-do-pregnancy-tests-work/). These can be from various reasons including [implantation](https://nabtahealth.com/glossary/implantation/) bleeding, cervical issues, [placenta](https://nabtahealth.com/glossary/placenta/) abnormalities, [ectopic pregnancies](https://nabtahealth.com/articles/ectopic-pregnancies-why-do-they-happen/), and miscarriages. In general, you will not get your period while you are pregnant. There is a small percentage of women who could have longer-than-usual periods and may continue to bleed, but will also be ovulating at the same time. If this occurs, you could technically be pregnant while on your period. However, you would not typically know at this stage because it would be extremely early (as in 1-3 days) into your pregnancy. With this exception, you will not get your period while you are pregnant. This is due to the fact that your body has a menstrual cycle when you have not conceived and when you do become pregnant, the hormone shift prevents [ovulation](https://nabtahealth.com/glossary/ovulation/) and therefore any further periods. What causes bleeding during pregnancy? -------------------------------------- Many women experience bleeding when they are pregnant and can mistake this for a period. It is important to be aware of all the reasons you could experience vaginal bleeding while pregnant. Then notify your physician if you think your bleeding is cause for concern. Possible causes of bleeding include: * [Implantation](https://nabtahealth.com/glossary/implantation/) Bleeding. This occurs when the fertilized egg implants in the [uterus](https://nabtahealth.com/glossary/uterus/). * [](https://nabtahealth.com/articles/what-is-an-ectopic-pregnancy/)[Ectopic Pregnancy](https://nabtahealth.com/glossary/ectopic-pregnancy/). This is a life-threatening event where a fertilized egg implants in another location instead of the [uterus](https://nabtahealth.com/glossary/uterus/). The degree of bleeding can vary but is often accompanied by pain on the right or left side of your lower abdomen, dizziness, and lightheadedness. * [Miscarriage](https://nabtahealth.com/glossary/miscarriage/). A [](https://nabtahealth.com/articles/causes-of-miscarriage/)[miscarriage](https://nabtahealth.com/glossary/miscarriage/) or [threatened](https://nabtahealth.com/articles/miscarriage-101/) [miscarriage](https://nabtahealth.com/glossary/miscarriage/) is a pregnancy that ends on its own without carrying to term. A [miscarriage](https://nabtahealth.com/glossary/miscarriage/) causes bleeding, which possibly has large blood clots in the blood. A woman will also experience uterine cramping. Other times, you may experience some mild spotting with brown or light pink blood throughout your pregnancy. This bleeding is typically very light. This could be due to cervical irritation or infection. Talk with your physician immediately if the bleeding starts to worsen. When should I be worried about bleeding during pregnancy? --------------------------------------------------------- Here are some important situations where you should be worried about bleeding during pregnancy: * If you are bleeding heavily or if the bleeding is accompanied by severe abdominal pain. * If you are bleeding and have experienced a fall or other trauma. * If you are bleeding and have a history of miscarriages or other complications in previous pregnancies. * If you are bleeding and are in the second trimester of pregnancy or later. If you are pregnancy or think you might be pregnant and experience bleeding with pain, it is recommended to consult a healthcare professional immediately. \_\_\_ Nabta is reshaping women’s healthcare. We support women with their personal health journeys, from everyday wellbeing to the uniquely female experiences of periods, fertility, pregnancy, and [](https://nabtahealth.com/glossary)[menopause](https://nabtahealth.com/glossary/menopause/). You can track your menstrual cycle and get [personalised support by using the Nabta app.](https://nabtahealth.com/our-platform/nabta-app/) Get in [touch](/cdn-cgi/l/email-protection#fa839b96969bba949b988e9b929f9b968e92d4999597) if you have any questions about this article or any aspect of women’s health. We’re here for you. **Sources:** * American Pregnancy Association * Am I Pregnant? Health * MYTH: You Can’t Get Your Period During Your Pregnancy. KidsHealth https://kidshealth.org/en/teens/period-pregnancy.html * Can You Still Have Your Period If You’re Pregnant? Parents * Can You Be Pregnant and Still Get Your Period? Powered by Bundoo® Edited by Nabta Health

As your [due date](https://nabtahealth.com/glossary/due-date/) nears, you might be wondering how your body decides one day that it is time to give birth. What exactly kicks things off, and why do some women give birth on their [due date](https://nabtahealth.com/glossary/due-date/) while others seem to stay pregnant forever until they are induced? The exact physiology behind the labor and how it occurs isn’t totally understood. But we do know a few key facts about how labor can start, and why it isn’t the same for everyone. [During your pregnancy](https://nabtahealth.com/articles/what-could-happen-to-your-skin-during-pregnancy/), your body is actively trying to prevent an early delivery. Certain hormones like [progesterone](https://nabtahealth.com/glossary/progesterone/), nitric oxide, and a few others keep your [uterus](https://nabtahealth.com/glossary/uterus/) from contracting and delivering too early. Some things can override this and activate labor prematurely. These include certain infections, a severe illness in the mother such as the flu, and bleeding from a placental abruption. Still others deliver early because their [cervix](https://nabtahealth.com/glossary/cervix/) is too short or weak, and for some women who are prone to preterm delivery, we have no good reason to explain why it happens. We have a theory that labor begins with an activation phase. Think of this as your body’s switch being given the green light to go into labor. Estrogen is thought to play a part in this: it makes the uterine cells that contract activate and be put on high alert. These cells are also now receptive to oxytocin, which is the hormone that makes them contract. The next phase is called the stimulation phase. This is when labor really gets going. Uterine [contractions](https://nabtahealth.com/glossary/contraction/) now happen because the hormones oxytocin and [](https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3081099/)[prostaglandins](https://nabtahealth.com/glossary/prostaglandins/) are released in your body telling the contraction cells in the [uterus](https://nabtahealth.com/glossary/uterus/) to get to work—and voila!—[contractions](https://nabtahealth.com/glossary/contraction/) begin! Your baby might have a role in starting labor too, though we aren’t completely sure. Certain hormones released by your baby eventually get converted to a form of estrogen, which helps with the activation phase mentioned earlier. In animals such as sheep, the role of the baby is much more certain when it comes to starting labor, but in humans, we still need to do more studies. So while we might not be totally sure when labor will begin and why it starts so early for some women and later in others, a few clues exist that show the important role of certain hormones. Another interesting fact is more women go into labor at night. It has been proposed that this is a holdover from our distant ancestors. Think of the cavewoman in labor. It is much easier for her to hide away and give birth (when she is much more vulnerable to an attack) in the dark of night. Therefore, something associated with the circadian rhythms of our bodies may be the reason labor starts more often when it is dark out! What are signs that labor is approaching? ----------------------------------------- Signs that labor is approaching can vary from person to person. However, some common signs include: * [Contractions](https://nabtahealth.com/glossary/contraction/): This is the most common and obvious sign of labor. [Contractions](https://nabtahealth.com/glossary/contraction/) are regular, painful uterine [contractions](https://nabtahealth.com/glossary/contraction/) that help to open the [cervix](https://nabtahealth.com/glossary/cervix/) and push the baby down the birth canal. * Water breaking: This is when the amniotic sac surrounding the baby ruptures and releases [amniotic fluid](https://nabtahealth.com/glossary/amniotic-fluid/). This can happen before or during labor. * Increased vaginal discharge: As the [cervix](https://nabtahealth.com/glossary/cervix/) dilates and thins out, the amount of vaginal discharge may increase. This can be clear, pink, or slightly bloody. * Pelvic pressure: Many women experience a feeling of pressure in the pelvis as the baby descends and the [cervix](https://nabtahealth.com/glossary/cervix/) dilates. * Back pain: Some women experience lower back pain as labor approaches. This can be due to the pressure of the baby’s head on the pelvis, or to the release of hormones that relax the ligaments in the pelvis. * Nausea and vomiting: Some women experience nausea and vomiting as labor approaches. This can be due to the increased hormone levels and the physical stress of labor. * Diarrhea: Many women experience diarrhea just before or during labor. This can be due to the release of hormones that relax the muscles in the intestines. **Sources:** * Gabbe SG et al * Obstetrics: Normal and Problem Pregnancies * 5th ed * Normal labor and delivery. Powered by Bundoo®

[Gestational Diabetes](https://nabtahealth.com/glossary/gestational-diabetes/) Mellitus (GDM) is a form of diabetes that develops during pregnancy. Prevalence rates range from 1% to 15%, depending on the population studied, although, worryingly, [one report](https://www.hamad.qa/EN/All-Events/mefqsh2017/presentations/Documents/Sunday/D6E6_Diabetes.pdf) has shown that over 20% of Qatari women are likely to develop the condition. This highlights the extent of the problem in the MENA region, as both obesity levels and diagnosed cases of type 2 diabetes continue to rise. Fortunately, knowing more about the condition and adopting lifestyle changes can reduce the likelihood of serious complications. Here are eight things you should know about GDM: **1. Diabetes occurs when you have elevated blood sugar, or glucose.** ----------------------------------------------------------------------- In diabetes, your body cannot use the sugar and carbohydrates it takes in as food to make energy. As a result, the extra glucose accumulates, causing damage to small blood vessels throughout the body. Parts of the body at risk include the kidneys, the extremities (hands and feet), and sensitive organs, such as the eyes. **2\. More than 70% of women with GDM have a [BMI](https://nabtahealth.com/glossary/bmi/) > 25.** -------------------------------------------------------------------------------------------------- Approximately half of all cases of GDM are solely attributable to pre-pregnancy obesity and women who are severely obese are 8 times more likely to develop GDM than those who have a [Body Mass Index](https://nabtahealth.com/what-is-body-mass-index-bmi/) ([BMI](https://nabtahealth.com/glossary/bmi/)) within the normal range. Being overweight is considered by many to be the most significant risk factor in the development of GDM. If left untreated, GDM and obesity in combination have a far greater impact on pregnancy outcome, increasing the likelihood of complications during delivery and adverse [neonatal](https://nabtahealth.com/glossary/neonatal/) effects. Obesity is a [modifiable risk factor](../how-can-i-reduce-my-risk-of-developing-gestational-diabetes), which means with the right support and a healthy diet, its detrimental effects can be reduced. This may require visiting a certified nutritionist to ensure you are still getting adequate calories and nutrition, particularly as diet is so important [prior to](../how-eating-the-right-food-might-help-you-to-conceive) and during pregnancy. **3. Ethnicity is one of the strongest non-modifiable risk factors for developing GDM.** ----------------------------------------------------------------------------------------- Worldwide the risk of developing GDM during pregnancy is thought to be approximately 10%. However, in certain [high risk populations](../ethnicity-and-gestational-diabetes) the risk is greater. Different studies have looked at different populations in detail and found that comparing across countries is challenging due to a lack of universally accepted diagnostic criteria and screening approaches. However, there are estimated prevalence rates for various Middle Eastern countries which range from 12.6% in Kuwait to 20.6% in the UAE. The prevalence of GDM amongst Asian Indians is thought to be 19.3%, which is higher than that seen for other Asian sub-populations. The prevalence of GDM across Europe, America and Australia is typically lower, for example, the average pregnant Swedish female has only a 0.4-1.5% risk of GDM. **4. Having a family member with diabetes type 2 increases a woman’s risk of developing GDM.** ----------------------------------------------------------------------------------------------- A study of women with GDM in Qatar, found an overall prevalence rate of 16.3%. Of these women, over 30% had a family history of diabetes. This association is probably due to both genetics and lifestyle factors. To read about some of the other risk factors for developing GDM click [here](../risk-factors-for-gestational-diabetes). **5. Mothers with GDM usually have heavier babies.** ----------------------------------------------------- Macosomia is the medical term for babies that weigh between 4 and 4.5 KG at birth, they are also referred to as ‘large for gestational age’. A large birth weight is considered to be the predominant consequence of intrauterine exposure to GDM. [](https://nabtahealth.com/articles/fetal-macrosomia-is-my-baby-too-big-to-deliver/)[Macrosomia](https://nabtahealth.com/glossary/macrosomia/) increases the likelihood of shoulder dystocia and birth injury during delivery. Interventional approaches, such as [induction](../) and [C-section](../) are sometimes implemented to reduce the risk of [macrosomia](https://nabtahealth.com/glossary/macrosomia/). [Birth weights](https://nabtahealth.com/articles/weight-gain-during-pregnancy-how-much-is-too-much/) above 4.5 KG are at significantly greater risk of [perinatal](https://nabtahealth.com/glossary/perinatal/) and infant mortality. **6. Women with GDM are at increased risk of developing [preeclampsia](https://nabtahealth.com/glossary/preeclampsia/) and other pregnancy complications.** ------------------------------------------------------------------------------------------------------------------------------------------------------------ Following a GDM diagnosis one of the things your doctor will monitor you particularly closely for is high blood pressure and protein in the urine, as these can be early warning signs of [](../what-is-preeclampsia)[preeclampsia](https://nabtahealth.com/glossary/preeclampsia/). [Preeclampsia](https://nabtahealth.com/glossary/preeclampsia/) is a potentially life-threatening condition that can cause your baby to stop growing and put you at risk of suffering seizures or even a stroke. As a result, if you suspect you have [preeclampsia](https://nabtahealth.com/glossary/preeclampsia/), you should seek medical help immediately and expect to be closely monitored for the remainder of your pregnancy. Other pregnancy complications include [](../)[polyhydramnios](https://nabtahealth.com/glossary/polyhydramnios/), which occurs when there is an excess of [amniotic fluid](https://nabtahealth.com/glossary/amniotic-fluid/), and premature delivery (which might be planned or spontaneous). **7\. A diagnosis of GDM during pregnancy, increases your risk of being diagnosed with type 2 diabetes after pregnancy.** -------------------------------------------------------------------------------------------------------------------------- It is thought that women who experience GDM are up to 7 times more likely to develop type 2 diabetes within the next decade than women who have had a healthy pregnancy. The main reason for this is probably prolonged obesity. Over 70% of women with GDM have an unhealthy [BMI](https://nabtahealth.com/glossary/bmi/) (>25), and are classified as overweight, obese or severely obese. Unless they do something about their excess weight, they are likely to remain overweight after delivery. Obese people are estimated to be up to 80 times more likely to develop type 2 diabetes than those who have a [BMI](https://nabtahealth.com/glossary/bmi/) in the normal range. Type 2 diabetes is a chronic condition that requires careful monitoring, diet adjustments and the possibility of taking lifelong medication (insulin). The risk can be reduced by making the right choices before, during, and after pregnancy. Consume lots of vegetables and whole grains, and have fresh fruit that does not have a high sugar content, such as berries and grapefruit. To prevent excessive weight gain during pregnancy avoid food and drink that has a high sugar content (fizzy drinks, fruit juice, biscuits and most desserts) . Exercising can also help to keep your glucose levels under control. However, if you are not used to undertaking physical activity, consult your doctor prior to beginning any exercise regime. **8. A GDM diagnosis can have long term effects on your child’s health.** -------------------------------------------------------------------------- Babies who are born to mothers with GDM are at increased risk of becoming overweight or obese during childhood or adolescence. They also have an increased risk of suffering from high blood pressure and impaired glucose tolerance, which, in turn, enhances the likelihood of them going on to develop type 2 diabetes. Recent work has even suggested that changes within the uterine environment can give rise to epigenetic modifications, potentially affecting not just your child, but their offspring and future generations. The take home message is that, if left untreated, GDM can affect the health of both [you](../i-have-gestational-diabetes-what-are-the-risks-to-me) and [your baby](../i-have-gestational-diabetes-what-are-the-risks-to-my-unborn-baby). For the 50% of women who have GDM because they are overweight, implementing a healthy, balanced diet and exercising regularly may well prove sufficient to reduce their [BMI](https://nabtahealth.com/glossary/bmi/) to the normal range. This will improve their overall health as well as keeping their blood glucose levels under control and reducing the likelihood of serious complications. If lifestyle adjustments do not sufficiently control your blood sugar levels, your doctor might prescribe [medication](../taking-diabetes-medication-during-pregnancy-is-it-safe) or insulin to reduce the risk of GDM-related complications affecting you or your unborn baby. Nabta is reshaping women’s healthcare. We support women with their personal health journeys, from everyday wellbeing to the uniquely female experiences of fertility, pregnancy, and [menopause](https://nabtahealth.com/glossary/menopause/). Get in [touch](/cdn-cgi/l/email-protection#8ef7efe2e2efcee0efecfaefe6ebefe2fae6a0ede1e3) if you have any questions about this article or any aspect of women’s health. We’re here for you. **Sources:** * Bellamy, L, et al. “Type 2 Diabetes Mellitus after [Gestational Diabetes](https://nabtahealth.com/glossary/gestational-diabetes/): a Systematic Review and Meta-Analysis.” _The Lancet_, vol. 373, no. 9677, 23 May 2009, pp. 1773–1779., doi:10.1016/S0140-6736(09)60731-5. * Bener, A, et al. “Prevalence of [Gestational Diabetes](https://nabtahealth.com/glossary/gestational-diabetes/) and Associated Maternal and [Neonatal](https://nabtahealth.com/glossary/neonatal/) Complications in a Fast-Developing Community: Global Comparisons.” _International Journal of Women’s Health_, vol. 3, 2011, pp. 367–373., doi:10.2147/IJWH.S26094. * “Diabetes and Obesity.” _Diabetes.co.uk_, [www.diabetes.co.uk/diabetes-and-obesity.html](http://www.diabetes.co.uk/diabetes-and-obesity.html). * “Diabetes in Qatar.” _Middle East Forum on Qulity and Safety in Healthcare 2017_, [www.hamad.qa/EN/All-Events/mefqsh2017/presentations/Documents/Sunday/D6E6\_Diabetes.pdf](http://www.hamad.qa/EN/All-Events/mefqsh2017/presentations/Documents/Sunday/D6E6_Diabetes.pdf). * Fadl, H E, et al. “Maternal and [Neonatal](https://nabtahealth.com/glossary/neonatal/) Outcomes and Time Trends of [Gestational Diabetes](https://nabtahealth.com/glossary/gestational-diabetes/) Mellitus in Sweden from 1991 to 2003.” _Diabetic Medicine_, vol. 27, no. 4, Apr. 2010, pp. 436–441., doi:10.1111/j.1464-5491.2010.02978.x. * Groof, Z, et al. “Prevalence, Risk Factors, and Fetomaternal Outcomes of [Gestational Diabetes](https://nabtahealth.com/glossary/gestational-diabetes/) Mellitus in Kuwait: A Cross-Sectional Study.” _Journal of Diabetes Research_, vol. 2019, no. 9136250, 3 Mar. 2019, doi:10.1155/2019/9136250. * Mitanchez, D, et al. “Infants Born to Mothers with [Gestational Diabetes](https://nabtahealth.com/glossary/gestational-diabetes/) Mellitus: Mild [Neonatal](https://nabtahealth.com/glossary/neonatal/) Effects, a Long-Term Threat to Global Health.” _The Journal of Pediatrics_, vol. 164, no. 3, Mar. 2014, pp. 445–450., doi:10.1016/j.jpeds.2013.10.076. * Moosazadeh, M, et al. “Family History of Diabetes and the Risk of [Gestational Diabetes](https://nabtahealth.com/glossary/gestational-diabetes/) Mellitus in Iran: A Systematic Review and Meta-Analysis.” _Diabetes & Metabolic Syndrome_, vol. 11, no. Suppl. 1, Nov. 2017, pp. S99–S104., doi:10.1016/j.dsx.2016.12.016. * Pu, J, et al. “Racial/Ethnic Differences in [Gestational Diabetes](https://nabtahealth.com/glossary/gestational-diabetes/) Prevalence and Contribution of Common Risk Factors.” _Paediatric and [Perinatal](https://nabtahealth.com/glossary/perinatal/) Epidemiology_, vol. 29, no. 5, Sept. 2015, pp. 436–443., doi:10.1111/ppe.12209. * Schwartz, N, et al. “The Prevalence of [Gestational Diabetes](https://nabtahealth.com/glossary/gestational-diabetes/) Mellitus Recurrence–Effect of Ethnicity and Parity: a Metaanalysis.” _American Journal of Obstetrics and Gynecology_, vol. 213, no. 3, Sept. 2015, pp. 310–317., doi:10.1016/j.ajog.2015.03.011. * Yuen, L, and V W Wong. “[Gestational Diabetes](https://nabtahealth.com/glossary/gestational-diabetes/) Mellitus: Challenges for Different Ethnic Groups.” _World Journal of Diabetes_, vol. 6, no. 8, 25 July 2015, pp. 1024–1032., doi:10.4239/wjd.v6.i8.1024. With support from Bundoo®

The greatest risk for a baby that is exposed to [Gestational Diabetes](https://nabtahealth.com/glossary/gestational-diabetes/) Mellitus affect the newborn (GDM) in utero is [**large birth weight**](https://nabtahealth.com/articles/how-your-weight-can-affect-your-pregnancy/), which is known medically as [](https://www.mayoclinic.org/diseases-conditions/fetal-macrosomia/symptoms-causes)[macrosomia](https://nabtahealth.com/glossary/macrosomia/). #### [Macrosomia](https://nabtahealth.com/glossary/macrosomia/) This refers to babies who weigh over 4 KG or are above the 90th centile. Quite apart from the [difficulties for the mother](../i-have-gestational-diabetes-what-are-the-risks-to-me) in delivering such a large baby, [macrosomia](https://nabtahealth.com/glossary/macrosomia/) can have serious health consequences for the neonate, including an increased risk of [**birth injury**](https://nabtahealth.com/articles/5-types-of-vaginal-tears-from-giving-birth-and-what-they-mean/) and, fortunately only in exceptional cases, early [neonatal](https://nabtahealth.com/glossary/neonatal/) death. #### Other risks There is a slightly increased risk of **[foetal malformations](https://nabtahealth.com/glossary/foetal-malformations/)**. However, this is thought to be primarily due to undiagnosed type 2 diabetes, rather than GDM itself. GDM-induced malformations occur when the condition has been diagnosed early on in pregnancy. Most women are not diagnosed until after 24 weeks and thus, the risk of their babies developing malformations is negligible. GDM does increase the likelihood of interventional approaches such as [induced labour](../https://nabtahealth.com/induction-of-labour/) and [C-section](https://nabtahealth.com/is-caesarean-considered-a-better-choice/), each of which has its own complications. Furthermore, if these intervention techniques are implemented before 37 weeks, the birth will be classed as [**premature**](https://nabtahealth.com/articles/anemia-in-premature-infants/) and the baby may require further monitoring and additional care. Whilst studies are yet to find a direct link between maternal GDM and infant respiratory distress, babies that are more than 4 KG at birth have an increased risk of **respiratory distress**. A major problem in managing this situation is that premature birth and [C-section](https://nabtahealth.com/articles/is-performing-a-c-section-better-than-inducing-labour/) delivery are additional risk factors for respiratory distress. Therefore, even if you take steps to avoid [macrosomia](https://nabtahealth.com/glossary/macrosomia/) and its associated issues, your baby might still need additional medical support at birth. #### Later health problems In addition to the risk of complications during pregnancy and delivery, having untreated GDM can predispose your child to **health problems later in life**. These include impaired glucose tolerance, high blood pressure and obesity, which in combination increase the chances of them developing type 2 diabetes themselves. GDM is not the only risk factor for these conditions; genetics and lifestyle exposure almost certainly play an important role too. [Breastfeeding](https://nabtahealth.com/benefits-of-breastfeeding/) is one way of counteracting some of these negative effects, as it has been shown to improve glucose tolerance and lower the risk of childhood obesity. It has also been suggested that GDM in the mother can increase the likelihood of the child having **attention deficiencies and delayed language** as they reach middle childhood, around the age of 7. The offspring of less educated women are more affected, suggesting a concurrent environmental or genetic element. Recent studies have revealed that babies born to mothers with [GDM](https://nabtahealth.com/articles/i-have-gestational-diabetes-what-are-the-risks-to-me/) have different bacteria present in their gut. This is known as an **altered [microbiome](https://nabtahealth.com/glossary/microbiome/) profile**. It is thought that the presence of specific bacteria in the gut of a neonate helps with the maturation of their immune system. Thus, a disruption in this [homeostasis](https://nabtahealth.com/glossary/homeostasis/) can have long term effects on the child’s ability to overcome infections and put them at increased risk of [metabolic disease](https://nabtahealth.com/glossary/metabolic-disease/) later in life. Most of these adverse effects can be significantly reduced by successful management of the mother’s GDM; further highlighting the importance of [identifying](../how-is-gestational-diabetes-diagnosed) and treating the condition as soon as possible. Nabta is reshaping women’s healthcare. We support women with their personal health journeys, from everyday wellbeing to the uniquely female experiences of fertility, pregnancy, and [menopause](https://nabtahealth.com/glossary/menopause/). Get in [touch](/cdn-cgi/l/email-protection#9ee7fff2f2ffdef0fffceafff6fbfff2eaf6b0fdf1f3) if you have any questions about this article or any aspect of women’s health. We’re here for you. **Sources:** * Bener, A, et al. “Prevalence of [Gestational Diabetes](https://nabtahealth.com/glossary/gestational-diabetes/) and Associated Maternal and [Neonatal](https://nabtahealth.com/glossary/neonatal/) Complications in a Fast-Developing Community: Global Comparisons.” _International Journal of Women’s Health_, vol. 3, 2011, pp. 367–373., doi:10.2147/IJWH.S26094. * Dionne, G, et al. “[Gestational Diabetes](https://nabtahealth.com/glossary/gestational-diabetes/) Hinders Language Development in Offspring.” _Pediatrics_, vol. 122, no. 5, Nov. 2008, pp. e1073–1079., doi:10.1542/peds.2007-3028. * Groof, Z, et al. “Prevalence, Risk Factors, and Fetomaternal Outcomes of [Gestational Diabetes](https://nabtahealth.com/glossary/gestational-diabetes/) Mellitus in Kuwait: A Cross-Sectional Study.” _Journal of Diabetes Research_, vol. 2019, no. 9136250, 3 Mar. 2019, doi:10.1155/2019/9136250. * Mitanchez, D. “Foetal and [Neonatal](https://nabtahealth.com/glossary/neonatal/) Complications in [Gestational Diabetes](https://nabtahealth.com/glossary/gestational-diabetes/): [Perinatal](https://nabtahealth.com/glossary/perinatal/) Mortality, Congenital Malformations, [Macrosomia](https://nabtahealth.com/glossary/macrosomia/), Shoulder Dystocia, Birth Injuries, [Neonatal](https://nabtahealth.com/glossary/neonatal/) Complications.” _Diabetes & [Metabolism](https://nabtahealth.com/glossary/metabolism/)_, vol. 36, no. 6, ser. 2, Dec. 2010, pp. 617–627. 2, doi:10.1016/j.diabet.2010.11.013. * Mitanchez, D, et al. “Infants Born to Mothers with [Gestational Diabetes](https://nabtahealth.com/glossary/gestational-diabetes/) Mellitus: Mild [Neonatal](https://nabtahealth.com/glossary/neonatal/) Effects, a Long-Term Threat to Global Health.” _The Journal of Pediatrics_, vol. 164, no. 3, Mar. 2014, pp. 445–450., doi:10.1016/j.jpeds.2013.10.076. * Su, M, et al. “Diversified Gut Microbiota in Newborns of Mothers with [Gestational Diabetes](https://nabtahealth.com/glossary/gestational-diabetes/) Mellitus.” _PloS One_, vol. 13, no. 10, 17 Oct. 2018, p. e0205695., doi:10.1371/journal.pone.0205695.

The risk factors for [Gestational Diabetes](https://nabtahealth.com/glossary/gestational-diabetes/) Mellitus (GDM) occurs when the body does not produce enough insulin and blood sugar levels get too high during [pregnancy](https://nabtahealth.com/articles/complications-during-pregnancy-polyhydramnios/). It most commonly occurs in the second and third trimester. Prevalence varies around the world, but with [obesity](https://nabtahealth.com/what-is-body-mass-index-bmi/) considered a major risk factor, and the number of obese females increasing, GDM is becoming a significant health issue of the 21st Century. Having [GDM](https://nabtahealth.com/articles/i-have-gestational-diabetes-what-are-the-risks-to-my-unborn-baby/) does increase the risk of complications for both mother and baby. However, the risks from GDM can be reduced if it is detected early and managed well. This article looks at what impact GDM has on the mother’s health; to see the risks to her offspring click [here](../i-have-gestational-diabetes-what-are-the-risks-to-my-unborn-baby). #### Pregnancy complications Women who are diagnosed with GDM are at increased risk of [pregnancy complications](https://nabtahealth.com/articles/complications-during-pregnancy-polyhydramnios/) including [](https://nabtahealth.com/complications-during-pregnancy-polyhydramnios/)[polyhydramnios](https://nabtahealth.com/glossary/polyhydramnios/), which occurs when there is an excess of [amniotic fluid](https://nabtahealth.com/glossary/amniotic-fluid/). They are also at increased risk of developing [hypertension](https://nabtahealth.com/glossary/hypertension/) (high blood pressure) and [](../what-is-preeclampsia)[preeclampsia](https://nabtahealth.com/glossary/preeclampsia/). [Preeclampsia](https://nabtahealth.com/glossary/preeclampsia/) is a life-threatening condition that requires close medical monitoring. In severe cases it can [lead](https://nabtahealth.com/glossary/lead/) to maternal seizures and will often result in premature delivery. #### Delivery In terms of delivery, women with GDM are more likely to experience [premature labour](https://nabtahealth.com/glossary/premature-labour/). In some cases this is spontaneous, but, in many cases, rapid growth of the baby in utero necessitates medical intervention. Babies born to mothers with GDM are frequently above the 90th percentile and if allowed to go to [full term](https://nabtahealth.com/glossary/full-term/) can weigh more than 4.5 KG at birth. Delivering such a large baby puts the mother at increased risk of complications and, therefore, [induced delivery](https://nabtahealth.com/induction-of-labour/) and planned [C-sections](https://nabtahealth.com/is-caesarean-considered-a-better-choice/) are common following a GDM diagnosis. The mother also has an increased risk of postpartum haemorrhage, which can be very dangerous if not attended to rapidly. #### Long-term health impact GDM can also have longer-term effects on the mother’s health. Women who are diagnosed with GDM are over 7 times more likely to develop [type 2 diabetes](https://nabtahealth.com/product/type-2-diabetes-starter-pack-copy/); most often in the first 5 years post-childbirth. Some women actually find that the GDM that is diagnosed during pregnancy persists after delivery and is reclassified as type 2 diabetes. The risk of a woman developing GDM during a subsequent pregnancy is approximately 48%, but can be significantly higher if she falls into a [high risk group](../risk-factors-for-gestational-diabetes). Nabta is reshaping women’s healthcare. We support women with their personal health journeys, from everyday wellbeing to the uniquely female experiences of fertility, pregnancy, and [menopause](https://nabtahealth.com/glossary/menopause/). Get in [touch](/cdn-cgi/l/email-protection#c6bfa7aaaaa786a8a7a4b2a7aea3a7aab2aee8a5a9ab) if you have any questions about this article or any aspect of women’s health. We’re here for you. **Sources:** * Bellamy, L, et al. “Type 2 Diabetes Mellitus after [Gestational Diabetes](https://nabtahealth.com/glossary/gestational-diabetes/): a Systematic Review and Meta-Analysis.” _The Lancet_, vol. 373, no. 9677, 23 May 2009, pp. 1773–1779., doi:10.1016/S0140-6736(09)60731-5. * Bener, A, et al. “Prevalence of [Gestational Diabetes](https://nabtahealth.com/glossary/gestational-diabetes/) and Associated Maternal and [Neonatal](https://nabtahealth.com/glossary/neonatal/) Complications in a Fast-Developing Community: Global Comparisons.” _International Journal of Women’s Health_, vol. 3, 2011, pp. 367–373., doi:10.2147/IJWH.S26094. * “[Gestational Diabetes](https://nabtahealth.com/glossary/gestational-diabetes/) (Overview).” _NHS_, [www.nhs.uk/conditions/gestational-diabetes/](http://www.nhs.uk/conditions/gestational-diabetes/). * Groof, Z, et al. “Prevalence, Risk Factors, and Fetomaternal Outcomes of [Gestational Diabetes](https://nabtahealth.com/glossary/gestational-diabetes/) Mellitus in Kuwait: A Cross-Sectional Study.” _Journal of Diabetes Research_, vol. 2019, no. 9136250, 3 Mar. 2019, doi:10.1155/2019/9136250. * Schwartz, N, et al. “The Prevalence of [Gestational Diabetes](https://nabtahealth.com/glossary/gestational-diabetes/) Mellitus Recurrence–Effect of Ethnicity and Parity: a Metaanalysis.” _American Journal of Obstetrics and Gynecology_, vol. 213, no. 3, Sept. 2015, pp. 310–317., doi:10.1016/j.ajog.2015.03.011.





























