3 Ways to Boost Milk Supply
Dr. Kate Dudek • July 3, 2025 • 5 min read

Following childbirth, many women that wish to breastfeed worry about their milk supply. Milk production is regulated by the hormones prolactin and oxytocin, which start working mid-way through pregnancy; however, once the baby is born, on-going production comes from consistent and regular removal of the milk from the breasts.
Therefore, the single best way of improving milk supply is to feed, or express, often. The first few days after delivery are critical for establishing milk secretion and this is the time at which many women who are struggling with breastfeeding decide to switch to formula feeding.
There are options for increasing milk supply and for those women who are struggling with breastfeeding, it may be worth trying these before switching to an entirely formula-based diet.
1. Seek professional help
Prior to attempting pharmacological methods or herbal remedies try speaking to an expert. Your gynaecologist or midwife should be able to put you in touch with a local lactation specialist. These women are trained to offer advice and counselling. They can evaluate whether your breastfeeding challenges are physical (for example, poor positioning, latching difficulties, baby tongue tie) or emotional (usually due to fluctuating hormone levels after giving birth). Their role is to support and encourage, and it is essential that if they do not do this, you find somebody else, who does.
2. Pharmacological galactogogues
A galactogogue is a substance administered to enhance milk supply. To date, there have been no drugs approved solely to enhance lactation. The medications that are prescribed are usually licensed for other purposes and used ‘off label’. That does not mean they are unsafe; as licensed drugs, they will have undergone extensive safety testing and, when prescribed to assist with lactation, they are given at a significantly lower dose than that normally recommended.
Domperidone is an antiemetic, sometimes given to infants with severe gastrointestinal reflux. Domperidone stimulates the release of prolactin, which is one of the hormones that regulate milk production. When given at a dose of 10 mg, three times a day, there is a modest increase in milk production; generally of between 80 and 100 mL a day.
There is an association between domperidone and cardiac arrhythmias and, in very rare cases, sudden cardiac death. Therefore, women with a history of heart complications should be advised against the use of this drug. It does not cross the blood-brain barrier, meaning there is no risk of neurological side effects, and the dose that passes into breast milk is extremely low. Given for the first few weeks post delivery, it is moderately successful at enhancing milk supply, but longer term studies on its efficacy are lacking.
Metoclopromide is an alternative medication sometimes used to stimulate milk production. Like domperidone, it’s primary usage is to prevent nausea and vomiting, but it also increases prolactin levels. Unlike domperidone, it crosses the blood-brain barrier and can cause quite severe neurological side effects, such as tremor and bradykinesia (slowness of movement).
Most studies on this drug have failed to find a significant increase in milk production. More of the drug passes into the breast milk, although levels are still well below those given therapeutically to infants with stomach complaints. The side effects and lower efficacy mean that, generally, domperidone is preferred over metoclopromide for improving lactation.
It is recommended that when medication is prescribed, women continue to feed and pump milk regularly to further enhance their supply.
3. Herbal galactogogues
Perhaps the best known non-pharmacological method of boosting milk supply is via the consumption of lactation cookies (or brownies, or lemonade, depending on personal preference). These can be homemade or shop-bought; however, the latter often come with a high price tag and indiscriminate ingredients, meaning their effectiveness may be questionable. It is the individual ingredients within lactation products that give them their proposed galactogogue properties.
The most widely known herbal remedy for enhancing milk supply is fenugreek seeds. As well as being a key ingredient in lactation cookies, these seeds can be consumed in capsule form or dissolved to make a tea. Fenugreek seeds have been used extensively as a cooking spice across India and the Middle East for many years. They stimulate sweat production and, as the mammary gland is a modified sweat gland, it is proposed that they stimulate this gland to produce milk.
The evidence for their efficacy is inconclusive and mainly anecdotal, although they do seem to have a mild galactagogue effect and many lactation consultants will recommend them. A dosage of 1 – 6 grams a day is recommended and side effects are generally minor, diarrhoea and flatulence being amongst the most common. At high doses, fenugreek can lower blood sugar levels, so it is suggested that women with diabetes mellitus do not use it.
There are other herbal options which include shatavari root, malunggay leaves and silymarin (65-80% milk thistle extract). Malunggay is widely used as a galactogogue in the Philippines and thistle extract is another common ingredient in lactation cookies. However, the scientific evidence for their beneficial qualities is lacking. There are very few studies, and the results are variable and inconclusive.
Herbal products do not need to undergo the same rigorous testing as other food and drink products. This means they are not regulated by government bodies and do not need to be tested on humans prior to being sold. The safety profiles of herbal products may not be as well established as conventional medication, however, many, including fenugreek seeds, have a long history of use in cooking and medicine, and therefore, are generally considered to be very safe and well tolerated.
In conclusion, adequate support, on both an emotional and practical level as well as frequent feeding (or expressing) are the best ways of boosting milk supply. Medical and herbal products seem to show some beneficial effects, however, the scientific evidence for their usage is limited and often restricted to short-term studies.
Nabta is reshaping women’s healthcare. We support women with their personal health journeys, from everyday wellbeing to the uniquely female experiences of fertility, pregnancy, and menopause.
Get in touch if you have any questions about this article or any aspect of women’s health. We’re here for you.
Seek more advice from at-home lactation consultation and get to learn more
Sources:
- Asztalos, E V. “Supporting Mothers of Very Preterm Infants and Breast Milk Production: A Review of the Role of Galactogogues.” Nutrients, vol. 10, no. 5, 12 May 2018, doi:10.3390/nu10050600.
- Bazzano, A N, et al. “A Review of Herbal and Pharmaceutical Galactagogues for Breast-Feeding.” The Ochsner Journal, vol. 16, no. 4, 2016, pp. 511–524.
- Drugs and Lactation Database (LactMed) [Internet]. Bethesda (MD): National Library of Medicine (US); 2006-. Fenugreek. [Updated 2019 May 1]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK501779/.
- Grzeskowiak, L E, et al. “Domperidone for Increasing Breast Milk Volume in Mothers Expressing Breast Milk for Their Preterm Infants: a Systematic Review and Meta‐Analysis.” BJOG, vol. 125, no. 11, Oct. 2018, pp. 1371–1378., doi:10.1111/1471-0528.15177.
Download the Nabta App


Related Articles

Why Does my Toddler Want to be Naked? (2024)
Find out why toddler want to be naked and get simple tips to manage it calmly, including sensory needs, new skills, and setting routines, The toddler years are marked by a variety of developmental milestones, one of which is the ability to dress and undress independently. While this new skill can be exciting for children, it can often [lead](https://nabtahealth.com/glossary/lead/) to inconvenient or embarrassing situations for parents, such as toddlers wanting to be naked all the time. However, this behavior is quite common and typically not a cause for concern. Why Toddlers Want to Be Naked ----------------------------- * **Sensory Input:** The main possible reasons toddlers like to keep naked include sensory input. Clothing such as seams within socks or shirt tags may be uncomfortable for a child, and this sensation of discomfort may make them remove their clothes frequently. If you suspect the child is extremely sensitive to a trivial input, it may indicate a problem like sensory processing disorder, for which the pediatrician can be consulted. * **Undressing as an Achievable Developmental Milestone**: One needs to consider that this might be one of the primary ways a toddler achieves a milestone in their development. They may feel proud of their new skill and want to share it with others, no matter how frustrating this may be for the parent. * **Attention Seeking**: The toddler may sometimes undress for attention; this is particularly true if the parent responds strongly to the behavior. The reaction from a frustrated or embarrassed parent may elicit persistence in undressing with the child to get some form of response. This, therefore, means that how parents react significantly influences behavior. How to Handle Your Toddler’s Nakedness -------------------------------------- * **Stay calm**: Parents should not react humiliatingly to the child instead of getting angry but may respond calmly with no humiliating remarks. The parents may tell their children how good they are at undressing and ask them to wear their clothes. This should be responding neutrally to avoid further exaggeration of the behavior. You might try dialogue like, “Wow! Terrific. I can see you undress yourself like a big kid. Can you get dressed now and show me how you do that?” By acting like the undressing is no more of a big deal than dressing, this may stop the problem in its tracks. * **Allocate Times to be Undressed**: At times, parents will find it beneficial to establish times when the toddler can be undressed, such as in preparation for bath time or within the confines of the home. More often than not, these organized opportunities will enable toddlers to feel less anxious and content with the parameters that have been established. * **Remember, It’s Just a Phase**: Like most [phases of development](https://nabtahealth.com/article/qa-with-raquel-anderson-brain-development-in-a-12-month-old/), the compulsion to be naked shall pass. Children do appear to grow out of it eventually, and parents need a little patience and understanding. **References:** 1.A. R. Turner, P. S. Thompson, “Sensory Processing and the Toddler Years: A Study of Early Childhood Sensory Experiences,” Journal of Developmental Psychology, 2023. 2.M. E. Calloway, J. L. Roberts, “Undressing as a Developmental Milestone in Early Childhood,” Infant and Toddler Development Journal, 2024. 3.S. D. Harris, “Understanding Toddler Behavior: Reactions to Nakedness and Sensory Sensitivity,” Parenting Psychology Quarterly, 2024. 4.L. B. Wilkins, “How to Respond to Common Toddler Behaviors: Positive Guidance Techniques,” Journal of Child Development and Parenting, 2023. **Sources:** * What To Expect * Undressing (preferring to be naked). [American Academy of Pediatrics](https://www.aap.org/) * Emotional Development in Preschoolers. Powered by Bundoo®

Fact or Fiction: Garlic Oil Helps Cure Ear Infections 2024
Garlic oil helps cure ear infections, natural [treatments](https://nabtahealth.com/) such as garlic oil are highly recommended as possessing antibacterial and antiviral properties. But does garlic oil live up to its reputation? The Science Behind Garlic and Ear Infections -------------------------------------------- Garlic has been used as a natural remedy for several centuries to cure various infections, among other ailments. The active ingredient, allicin, has been shown to exhibit antibacterial and antiviral properties that can help with the symptoms of an ear infection. A few studies confirm that allicin decreases the presence of certain bacteria and viruses, thus assisting in resolving the ear infection sooner. Yet anatomically, the ear makes this problematic as the tympanic membrane, or eardrum, acts to prevent direct delivery of oil or drops to the area of the middle ear where infections occur. 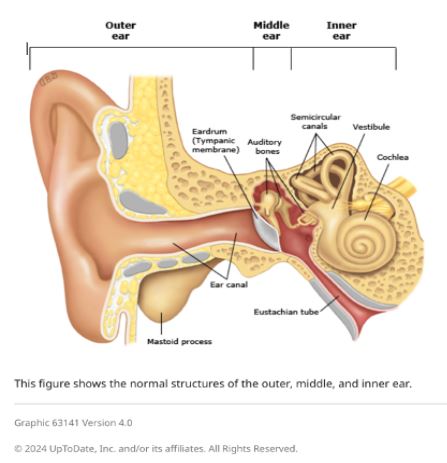 Evidence of Garlic Oil and Herbal Remedies ------------------------------------------ Studies on garlic oil, often combined with other herbs such as mullein, demonstrate it can decrease ear pain. A review published in 2023 reported that herbal ear drops, including those containing garlic, relieved pain in subjects with acute otitis media. However, researchers pointed out that while garlic oil may grant some advantages in the feeling of discomfort, its effect on the infection is limited by the eardrum barrier. Most infections will still self-resolve, but garlic oil can offer a natural alternative for pain management. Some studies in 2023 and 2024 also report that herbal extracts, including garlic, reduce dependence on heavy pain medications. Garlic is relatively cheaper and easier to access in herbal drops, particularly in many settings where prescription ear drops are not available. Safety and Proper Application of Garlic Oil ------------------------------------------- Being a potentially palliative resource, garlic needs to be used in the right manner. Experts advise against putting pure or undiluted garlic oil into the ear, as this can be too harsh and thus irritate or even injure sensitive ear tissue. Garlic extracts in commercially prepared herbal ear drops are recommended for use in the ear. In these products, garlic would have been diluted to safe levels while still being beneficial. Seeing a Health Professional ---------------------------- Consulting a health professional beforehand is very important when using garlic oil or any other herbal remedy against ear infections. Sometimes, ear infections result in complications, especially when not treated properly, and might cause recurrence. A healthcare provider will best help assess whether garlic oil or any other remedy may be indicated for each case and may recommend the safest treatment. Possible Benefits of Garlic Oil for Ear Health ---------------------------------------------- * Natural Pain Relief: Garlic oil’s antimicrobial and anti-inflammatory action soothes ear pain. * Cost-Effective: Garlic-based herbal remedies are generally cheaper than several prescription-based ear drops. * Readily Available Option: Garlic oil is readily available at health stores and can be ordered online. Current Research and Future Directions -------------------------------------- Herbal remedies, such as garlic oil, are still under research, especially for their role in pain relief and supporting natural recovery in light ear infections. Other studies investigate more advanced formulations that could let active compounds bypass the eardrum more effectively, thus giving a chance for enhanced effectiveness against middle-ear infections without the use of antibiotics. Key Takeaways ------------- * In effect, it has a minimal impact on the infection. It does not cure the disease but helps with earache because the membrane prevents the oil from reaching the middle ear. * Only use mild formulations. Commercially prepared herbal ear drops are very good compared to undiluted garlic oil. This is done to prevent irritation. * Consult a professional. Consult your health provider before this natural remedy, especially if you have recurring symptoms. References 1.Johnson, L., & Patel, R. (2023). [The Role of Herbal Remedies in Treating Ear Pain](https://pubmed.ncbi.nlm.nih.gov/): A Focus on Garlic Oil. Journal of Complementary Medicine, 61(2), 102-115. 2.Sharma, D., & Lee, H. (2024). Evaluating Garlic Extract for Natural Pain Relief in Ear Infections. Advances in Integrative Health, 42(1), 89-99. 3.Verhoeven, E., & Kim, S. (2023). Garlic and Herbal Extracts in Ear Infection Management. Health and Wellness Journal, 23(4), 167-178.

Is Performing a C-Section Better Than Inducing Labour? [2024]
Is Performing a C-Section Better Than Inducing Labour, when it comes to giving birth, usually the preferred option is to let labour proceed naturally. However, there are times when it is not in the mother or baby’s interest for this to happen. When the health of either is at risk, or if gestation has exceeded [41 weeks duration,](https://nabtahealth.com/articles/doctor-tips-weeks-27-40/) then it is highly probable that an alternative strategy will need to be implemented. There are two options available, [inducing labour](../) or performing a [C-section](../). With an induction, the [uterus](https://nabtahealth.com/glossary/uterus/) is artificially stimulated to contract, and it is then hoped that labour will proceed as per a natural delivery. In contrast, a C-section is a surgical procedure, whereby a cut is made in the abdomen and the baby is removed that way, rather than via the [vagina](https://nabtahealth.com/glossary/vagina/). Sometimes the only safe option is to perform a C-section, for example if the baby is breach, or when an emergency situation arises. However, there are other times when you may be presented with a choice and if this happens, what is the correct answer? Unfortunately there is no definitive right answer. An induction can be at least as safe as spontaneous labour and, if performed in the week prior to the [due date](https://nabtahealth.com/glossary/due-date/), it is thought to reduce [the risk of](https://nabtahealth.com/articles/what-is-preeclampsia/) [preeclampsia](https://nabtahealth.com/glossary/preeclampsia/) in the mother and respiratory distress in the child, possibly as a result of the [placenta](https://nabtahealth.com/glossary/placenta/) remaining fully functional. Unlike C-sections, inductions are not surgical procedures and thus, if all goes to plan, the recovery period is shorter. It is however, a big ‘IF’. [Induced labours](https://nabtahealth.com/articles/induction-of-labour/) are typically more painful, meaning more women will request stronger pain relief including epidurals, and there is a greater likelihood of assisted delivery, such as the use of forceps or ventouse. There is also an increased [risk of hyperstimulation](https://nabtahealth.com/articles/what-is-ovarian-drilling/) of the [uterus](https://nabtahealth.com/glossary/uterus/)., Uterine hyperstimulation causes more frequent, longer [contractions](https://nabtahealth.com/glossary/contraction/), which can [lead](https://nabtahealth.com/glossary/lead/) to complications such as foetal heart rate abnormalities and, in rare cases, uterine rupture. In a significant number of women, induction does not work and a C-section becomes necessary. The advent of the C-section was undoubtedly a medical revolution, instantly saving the lives of millions of women and children. However, C-sections bring with them all the risks of regular surgery, including blood clots, wound infection and bleeding. The recovery period is typically longer after a C-section than after a natural birth, driving restrictions are enforced and a scar remains, although this will fade over time. Whilst current guidelines stipulate that an induction should only be performed when [the risks of continuing the pregnancy](https://nabtahealth.com/articles/complications-during-pregnancy-polyhydramnios/) outweighs the benefits, with more women than ever requesting elective C-sections, the World Health Organisation has highlighted an urgent need for medical assessment efforts to address the risks of induced labour compared to elective C-section. Until such work is undertaken, it becomes a matter of individual circumstance, personal choice and ultimately weighing up what is best for you and your baby. **Sources:** * Grobman, W A, et al. “Labor Induction versus Expectant Management in Low-Risk Nulliparous Women.” _The New England Journal of Medicine_, vol. 379, no. 6, 9 Aug. 2018, pp. 513–523., doi:10.1056/NEJMoa1800566. * WHO Recommendations for Induction of Labour. World Health Organisation, [http://apps.who.int/iris/bitstream/handle/10665/44531/9789241501156\_eng.pdf?sequence=1](http://apps.who.int/iris/bitstream/handle/10665/44531/9789241501156_eng.pdf?sequence=1). Accessed on 23/01/2019. * _Inducing Labour. Clinical Guideline \[CG70\]_. NICE (National Institute for Care and Health Excellence), July 2008, www.nice.org.uk/guidance/cg70/chapter/Introduction. Accessed on 23/01/2019