نصحني طبيبي بإجراء استئصال بطانة الرحم؛ ما الذي يجب أن أعرفه؟
Ablation of the endometrium is a gynaecological procedure that has been in use since the late 19th century. The aim of the procedure is to control vaginal bleeding without the need for a hysterectomy. It works by destroying (ablating) the lining of the uterus (endometrium).
When will an endometrial ablation be recommended?
Endometrial ablations are generally recommended to those women who experience prolonged bouts of heavy menstrual bleeding. They are rarely the first approach as most doctors will be keen to reduce blood loss using medications or an intrauterine device (IUD) first.
Your doctor might recommend an endometrial ablation if your:
- Periods are so heavy that your pad or tampon needs changing every two hours.
- Blood loss is putting you at risk of becoming anaemic.
- Periods regularly last for longer than eight days (defined as abnormal uterine bleeding).
Whilst not used for sterilisation, most women who undergo the procedure end up infertile, so you should not have an endometrial ablation if you intend to have children in the future. Pregnancies that follow endometrial ablations are very high risk and can be ectopic or end in miscarriage.
How is an endometrial ablation performed?
Once you and your doctor have decided that an endometrial ablation is the best option for you, he or she will first of all want to rule out any possibility of pregnancy. Assuming a pregnancy test comes back negative, your doctor will prepare you for the procedure. Sometimes medications are given or a dilation and curettage (D&C) is performed to thin the endometrium, prior to the ablation.
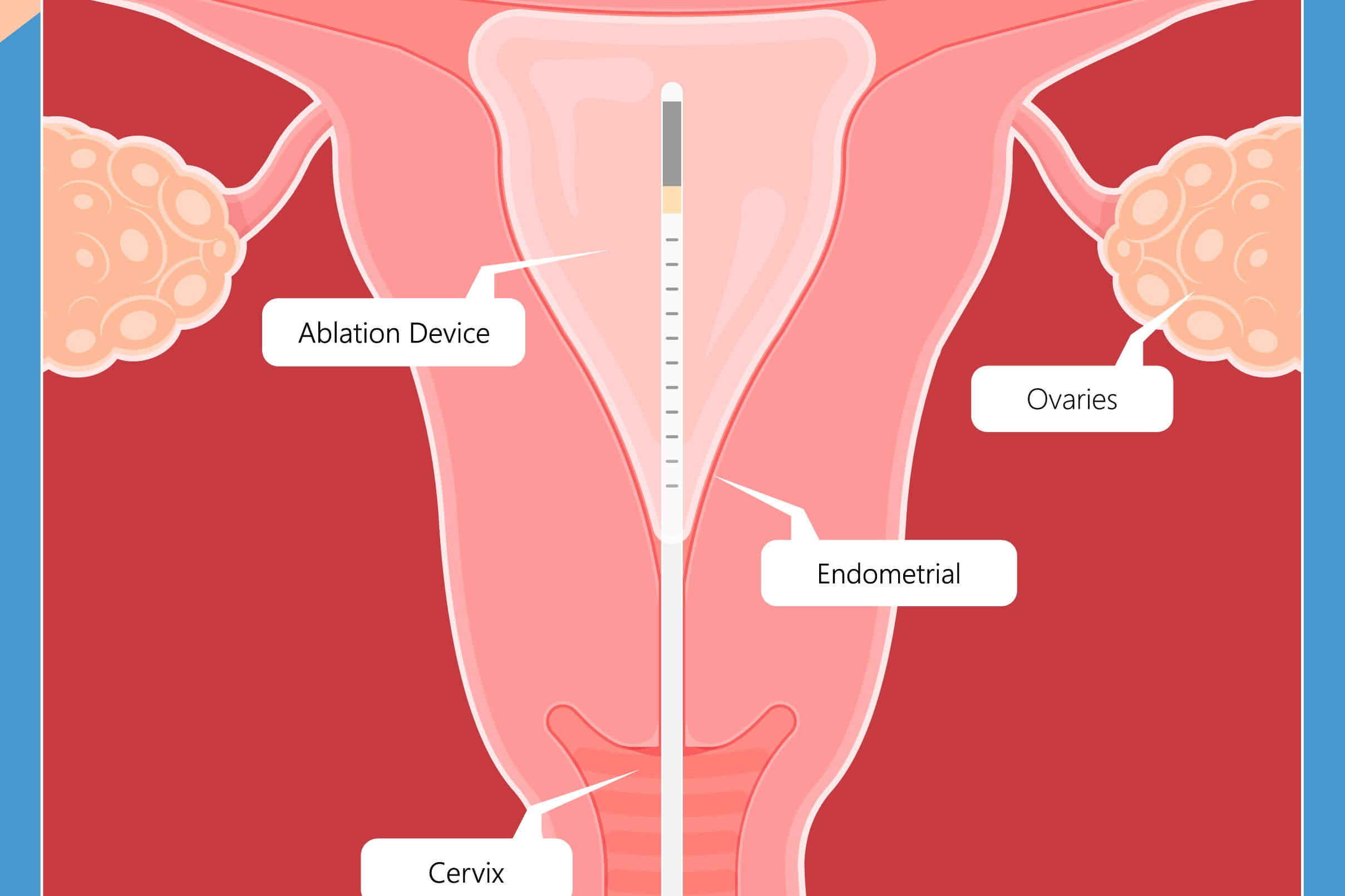
Advances in modern medicine have meant that many endometrial ablations carried out today can be performed as outpatient procedures and you will be able to go home the same day. Unlike some of the more invasive gynaecological techniques, a uterine ablation does not require any incisions to be made to the abdomen. Instead, the required tools are passed through the vagina and cervix to reach the uterus.
The first stage is to gently widen (dilate) the cervix using a series of rods to increase the diameter. This will give your doctor the room to maneuver whichever instruments he/she is using. A hysteroscope will usually be inserted to enable the doctor to see the inside of the uterus and sometimes carbon dioxide gas will be used to expand the uterus for the duration of the procedure.
The exact method used will depend on the size and condition of your uterus, as well as resource availability.
Types of endometrial ablation
- Electrosurgery (electrocautery): A wire loop is heated with an electric current and passed into the uterus. Once there, it carves furrows into the endometrium. Requires general anaesthetic.
- Cryoablation: Extreme cold is used to create ice balls that destroy the lining of the uterus. Each freeze cycle lasts about 6 minutes and the number of cycles required will depend on the size and shape of the uterus. Real-time ultrasound is used to track the state of the endometrium throughout.
- Free-flowing hot fluid: Saline solution, heated to between 80 and 90°C is circulated within the uterus for about 10 minutes. This is ideal for women who have an irregular shaped uterus, or one distorted by abnormal tissue growth, for example, fibroids.
- Heated balloon: A balloon device is inserted through the cervix and inflated once in the uterus, using fluid heated to 87°C. The procedure takes between two and ten minutes, depending on the condition and size of the uterus.
- Microwave: A slender tool is inserted through the cervix. Once in place, it emits microwaves to heat and destroy the endometrial tissue. The usual duration for this procedure is 3-5 minutes.
- Radiofrequency: A flexible, mesh device is inserted into the uterus, where it transmits radiofrequency energy that vaporises the endometrial tissue within a couple of minutes.
Some doctors will advocate a partial endometrial ablation, whereby only part of the endometrial wall is destroyed. This is with a view to reducing the number of late-onset complications seen with total ablations. Up to a quarter of women who have an endometrial ablation will end up needing a hysterectomy and this is particularly true for younger women. Preliminary data suggests that partial ablations have no long-term complications and result in improved quality of life scores and fewer hysterectomies. However, larger studies are required to validate this finding.
Do endometrial ablations work?
Approximately 80% of women see a reduction in menstrual blood loss following endometrial ablation. Documented risks, such as damage to nearby organs and puncturing of the uterine wall occur very rarely and few women report procedure-related complications. Side effects are minimal; cramps, which can last a few days, and a watery, bloody vaginal discharge and increased need to pass urine, which usually passes within 24 hours.
Overall, the procedure is considered safe, effective and minimally invasive. It has reduced hysterectomy rates and improved the quality of life for many women trapped in a cycle of relentless heavy periods.
Try Nabta’s post-surgery pack after the procedure.
Nabta is reshaping women’s healthcare. We support women with their personal health journeys, from everyday wellbeing to the uniquely female experiences of fertility, pregnancy, and menopause.
Get in touch if you have any questions about this article or any aspect of women’s health. We’re here for you.
Sources:
- “Endometrial Ablation.” Johns Hopkins Medicine, www.hopkinsmedicine.org/health/treatment-tests-and-therapies/endometrial-ablation.
- “Endometrial Ablation.” Mayo Clinic, Mayo Foundation for Medical Education and Research, 8 Sept. 2018, www.mayoclinic.org/tests-procedures/endometrial-ablation/about/pac-20393932.
- Laberge, Philippe, et al. “Endometrial Ablation in the Management of Abnormal Uterine Bleeding.” Journal of Obstetrics and Gynaecology Canada, vol. 37, no. 4, 1 Apr. 2015, pp. 362–376., doi:10.1016/s1701-2163(15)30288-7.
- Mccausland, Vance, et al. “Partial Endometrial Ablation: A 10–20-Year Follow-Up of Impact on Bleeding, Pain, and Quality of Life.” Journal of Gynecologic Surgery, vol. 32, no. 4, 22 July 2016, pp. 230–235., doi:10.1089/gyn.2016.0012.
- Wortman, Morris. “Late-Onset Endometrial Ablation Failure.” Case Reports in Women’s Health, vol. 15, July 2017, pp. 11–28., doi:10.1016/j.crwh.2017.07.001.